Pharmacokinetics explains how drugs move through the body, but many nursing students memorize ADME without connecting it to real clinical care.
That is the problem.
In nursing pharmacology, pharmacokinetics is not just a definition to remember for an exam. It helps students understand why medication timing matters, why one route works faster than another, why kidney and liver function affect medication safety, why some drugs need closer monitoring, and why nurses reassess patients after medication administration.
This guide explains pharmacokinetics, ADME, absorption, distribution, metabolism, excretion, bioavailability, first-pass metabolism, half-life, onset, peak, duration, therapeutic range, steady state, clearance, patient factors, nursing responsibilities, and how to discuss these concepts in nursing assignments.
Quick Answer: What Is Pharmacokinetics?
- Pharmacokinetics describes how the body absorbs, distributes, metabolizes, and excretes a drug.
- The four main processes are ADME: absorption, distribution, metabolism, and excretion.
- Pharmacokinetics helps nurses understand medication timing, onset, peak effect, duration, half-life, and monitoring needs.
- Pharmacodynamics is different: it explains what the drug does to the body.
- Patient factors such as age, kidney function, liver function, circulation, body composition, and drug interactions can affect pharmacokinetics.
- Nurses use pharmacokinetic concepts to monitor therapeutic effects, adverse effects, toxicity risks, and medication timing.
- Students should understand pharmacokinetics as clinical reasoning, not just vocabulary.
What Is Pharmacokinetics?
Pharmacokinetics is the study of what the body does to a drug after it enters the body. It describes how a drug is absorbed into the bloodstream, distributed to tissues, changed by metabolism, and removed through excretion. These four processes are often summarized as ADME: absorption, distribution, metabolism, and excretion (Ernstmeyer & Christman, 2023; Patel & Barvaliya, 2023).
A simple way to remember it is:
Pharmacokinetics = what the body does to the drug.
For nursing students, this matters because medication administration does not end when a medication is given. A nurse must also think about when the medication may start working, when the patient may need reassessment, what adverse effects may occur, whether lab values matter, and whether the patient’s age, kidney function, liver function, hydration, or circulation could change the response.
Nurses do not prescribe medications in most clinical roles, and they should not independently change doses, routes, or medication schedules unless that action falls within their scope, training, policy, and provider orders. However, nurses still need pharmacokinetic knowledge because they administer many medications, observe patient responses, recognize safety concerns, and communicate changes to the healthcare team.
For example, if a patient receives a pain medication, the nurse should understand that the medication has an expected onset, peak effect, and duration. If the nurse reassesses too early, the medication may not have had enough time to work. Suppose the nurse fails to reassess around the expected peak, important adverse effects or therapeutic responses may be missed.
Pharmacokinetics helps connect medication knowledge to safe nursing judgment.
Pharmacokinetics vs Pharmacodynamics
These two are closely related, but they answer different questions.
Pharmacokinetics asks: How does the body move and process the drug?
Pharmacodynamics asks: What does the drug do to the body?
Pharmacokinetics focuses on drug concentration over time. It explains absorption, distribution, metabolism, excretion, bioavailability, half-life, clearance, and how long a drug may remain active in the body. Pharmacodynamics focuses on the drug’s effect, such as receptor activity, therapeutic response, adverse effects, side effects, and toxicity (Ernstmeyer & Christman, 2023; Patel & Barvaliya, 2023).
| Concept | Main question | Main focus | Nursing example | Student takeaway |
|---|---|---|---|---|
| Pharmacokinetics | What does the body do to the drug? | Absorption, distribution, metabolism, excretion, half-life, clearance | A nurse considers kidney function before monitoring for drug accumulation concerns. | It explains drug movement and concentration over time. |
| Pharmacodynamics | What does the drug do to the body? | Drug action, receptor response, therapeutic effect, adverse effect | A nurse monitors whether a medication lowers pain, blood pressure, fever, or inflammation. | It explains the drug’s effect on the patient. |
| Both together | Is the medication producing the expected effect safely? | Drug movement plus drug response | A nurse monitors both therapeutic response and adverse effects after administration. | Safe medication monitoring requires both concepts. |
A common student mistake is treating these two concepts as interchangeable. They are not the same. A drug may reach the bloodstream, but the patient’s response depends on both how the body handles the drug and how the drug acts on body systems.
Pharmacodynamics Overview: How Drug Effects Differ From Drug Movement
Pharmacodynamics explains how a medication produces effects in the body. While pharmacokinetics focuses on movement, pharmacodynamics focuses on action.
Many medications work by interacting with receptors. A receptor is a target site where a drug can bind and produce or block a response. An agonist activates a receptor and produces an effect. An antagonist blocks a receptor or prevents another substance from activating it. This is a basic explanation, but it helps nursing students understand why different medications can stimulate, reduce, block, or modify body responses.
Pharmacodynamics also includes the dose-response relationship. This means that changes in drug exposure may affect the intensity of response, although the relationship is not always simple or identical in every patient. Patient condition, receptor sensitivity, tolerance, interactions, age, organ function, and disease processes can all affect response.
Important pharmacodynamic terms include therapeutic effect, side effect, adverse effect, and toxicity. The therapeutic effect is the intended clinical effect. A side effect is an unintended effect that may occur at usual therapeutic use. An adverse effect is harmful or undesirable. Toxicity occurs when drug exposure or patient sensitivity leads to dangerous effects.
Potency and efficacy are also pharmacodynamic ideas. Potency refers to how much drug is needed to produce an effect. Efficacy refers to the maximum effect a drug can produce.
This section is only an overview. The main focus of this article remains pharmacokinetics: how drug movement affects timing, concentration, monitoring, and safety.
ADME in Pharmacokinetics
ADME stands for absorption, distribution, metabolism, and excretion. These four processes describe the general path of a drug through the body.
Students often memorize ADME as four separate words, but in the body, these processes connect. A medication may be absorbed from the gastrointestinal tract, distributed through the bloodstream, metabolized by the liver, and excreted by the kidneys. At the same time, some drug molecules may still be absorbing while others are already being metabolized or excreted.
That is why ADME is not just a list. It is a clinical framework.
| ADME process | Meaning | Nursing relevance | Simple example |
|---|---|---|---|
| Absorption | Drug enters the bloodstream | Affects onset, route considerations, and patient teaching | Oral medication may absorb more slowly than some non-oral routes. |
| Distribution | Drug moves from blood to tissues | Affected by perfusion, protein binding, fluid shifts, and body composition | Low albumin may affect highly protein-bound medications. |
| Metabolism | Body chemically changes the drug | Often involves liver function and drug interactions | Liver impairment may increase medication safety concerns. |
| Excretion | Drug leaves the body | Often depends on kidney function, urine output, and clearance | Reduced renal function can increase accumulation risk for some drugs. |
ADME helps nursing students organize medication thinking. Instead of asking only, “What is this drug for?” students should also ask, “How does this drug enter the body, where does it go, how is it changed, and how does it leave?”
Absorption: How Drugs Enter the Bloodstream
Absorption is the movement of a drug from the site of administration into the bloodstream. For many medications, absorption is the first major step before the drug can produce a systemic effect.
Drug absorption depends on several factors. These may include the route of administration, formulation, blood flow to the absorption site, gastrointestinal function, food, pH, skin condition, perfusion, and the patient’s overall clinical state (Alagga & Gupta, 2024).
Route matters because drugs enter the body in different ways. Oral medications usually pass through the gastrointestinal tract before reaching systemic circulation. Sublingual and buccal medications may absorb through mucous membranes. Transdermal medications absorb gradually through the skin. Inhaled medications may act locally in the respiratory tract or be absorbed systemically depending on the medication. Parenteral medications enter the body outside the digestive tract. IV administration bypasses absorption in the usual sense because the medication enters circulation directly.
Absorption affects onset and sometimes the intensity of effect. A medication that absorbs slowly may take longer to produce a noticeable response. A medication that absorbs rapidly may have a faster onset, although the clinical effect still depends on the drug, formulation, patient condition, circulation, and pharmacodynamics.
Nursing relevance is practical. Before giving medication, nurses verify the ordered route and consider whether patient factors could interfere with safe administration or expected absorption. For example, vomiting, swallowing difficulty, NPO status, poor perfusion, altered skin integrity, gastrointestinal dysfunction, or incorrect timing with food may matter depending on the medication and order.
For nursing students, the key point is this: absorption is not just “drug gets in.” It helps explain why route, formulation, timing, and patient condition matter.
For a fuller discussion of route differences, see the related guide on Medication Administration Routes.
Bioavailability and First-Pass Metabolism
Bioavailability refers to the amount or fraction of a drug that reaches systemic circulation in an active form. If less active drug reaches circulation, the expected effect may differ from a route or formulation that delivers more active drug into the bloodstream (Price & Patel, 2023).
IV medications are generally considered to have complete systemic bioavailability because the drug enters the bloodstream directly. Oral medications often have lower or more variable bioavailability because they must pass through the gastrointestinal tract and may be affected by absorption barriers, food, stomach emptying, intestinal metabolism, and first-pass metabolism.
First-pass metabolism is metabolism that occurs before the active drug reaches systemic circulation. It is commonly associated with the liver after gastrointestinal absorption, although metabolism can also involve other tissues (Herman & Santos, 2023; Susa et al., 2023).
In simple terms, first-pass metabolism can reduce the amount of active drug available to circulate through the body. This is one reason route matters.
Some routes may avoid or reduce first-pass effects depending on the medication and formulation. Sublingual, buccal, transdermal, and some parenteral routes may allow medication to enter systemic circulation without the same initial liver processing associated with many oral medications.
The nursing relevance is safety and accuracy. Nurses should not switch routes because routes are not automatically equivalent. The same medication may behave differently when given by different routes or formulations. Route changes require appropriate authorization, facility policy, drug reference guidance, and provider orders.
A common student mistake is assuming that the drug name alone tells the whole story. It does not. The route and formulation can strongly affect bioavailability, onset, intensity, and monitoring needs.
Distribution: How Drugs Move Through the Body
Distribution is the movement of a drug from the bloodstream into tissues and body compartments. After a drug reaches circulation, it does not affect every tissue equally. Distribution depends on blood flow, tissue characteristics, protein binding, body composition, and barriers such as the blood-brain barrier (Onetto & Sharif, 2023).
Highly perfused organs may receive drug exposure faster than poorly perfused tissues. This matters in patients with altered circulation, shock, edema, dehydration, heart failure, or critical illness. If tissue perfusion changes, drug movement may also change.
Protein binding is another important concept. Some drugs bind to plasma proteins such as albumin. Only the unbound portion of a drug is usually available to move into tissues and produce effects. If albumin is low, the amount of free drug may change for highly protein-bound medications. Nursing students do not need advanced calculations here, but they should understand why low albumin can matter in medication monitoring.
Body composition also affects distribution. Some medications distribute more into body water, while others distribute more into fat tissue. Older adults may have changes in body water, lean mass, fat composition, and protein levels, which can affect drug distribution.
The blood-brain barrier can limit the movement of some drugs into the central nervous system. Pregnancy and lactation also raise general distribution considerations because some medications may cross the placenta or enter breast milk, depending on the drug and patient context.
Nursing relevance includes monitoring older adults, patients with low albumin, patients with fluid shifts, critically ill patients, and patients with altered perfusion. Distribution helps explain why two patients may receive the same medication category but show different responses or adverse effects.
Metabolism: How the Body Changes Drugs
Metabolism is the chemical change of a drug within the body. The liver is the major organ involved in many drug metabolism processes, although metabolism can occur in other tissues as well (Susa et al., 2023).
Metabolism may inactivate a drug, activate a drug, or change it into metabolites that are easier to excrete. Some metabolites are inactive. Others remain active. Some drugs are given as prodrugs, meaning they need metabolism to become active.
Hepatic metabolism often involves enzymes. Nursing students do not need to memorize every enzyme system at the beginning level, but they should understand that enzyme activity can affect drug levels. If metabolism is slowed, drug levels may rise or last longer. If metabolism is increased, drug exposure may decrease for some medications.
Several factors can affect metabolism:
- liver disease
- age
- genetics
- alcohol use
- drug interactions
- nutritional status
- hepatic blood flow
- critical illness
The nursing relevance is monitoring. If a patient has liver impairment, abnormal liver-related labs, heavy alcohol use, multiple medications, or signs of adverse effects, the nurse should recognize possible medication safety concerns and communicate according to policy.
A common student confusion is thinking metabolism means “the drug leaves the body.” Metabolism changes the drug. Excretion removes the drug or metabolites. These processes often work together, but they are not identical.
Excretion: How Drugs Leave the Body
Excretion is the removal of drugs or drug metabolites from the body. The kidneys are a major route of excretion for many medications and metabolites. Other routes may include bile, feces, lungs, sweat, saliva, and breast milk, depending on the substance (Garza et al., 2023).
Renal function matters because impaired kidney function can reduce drug elimination for medications that depend on renal excretion. If a drug or active metabolite is not cleared as expected, accumulation may occur. Accumulation can increase the risk of adverse effects or toxicity, especially with repeated doses or narrow therapeutic range medications.
Creatinine clearance and estimated glomerular filtration rate, often written as eGFR, are common ways clinicians evaluate kidney function. Nursing students do not need to perform pharmacokinetic dose-adjustment calculations in this article. However, they should understand that renal function helps the healthcare team evaluate medication safety.
Factors that may affect excretion include kidney disease, older age, hydration status, urine output, renal perfusion, and drug interactions. A patient with dehydration, poor perfusion, or reduced urine output may have different excretion concerns from a stable patient with normal renal function.
Nursing relevance includes checking ordered labs, monitoring urine output where appropriate, observing for adverse effects, identifying toxicity concerns, and communicating changes to the healthcare team. Nurses should not independently adjust medication doses, but they should recognize when patient changes may make medication monitoring more important.
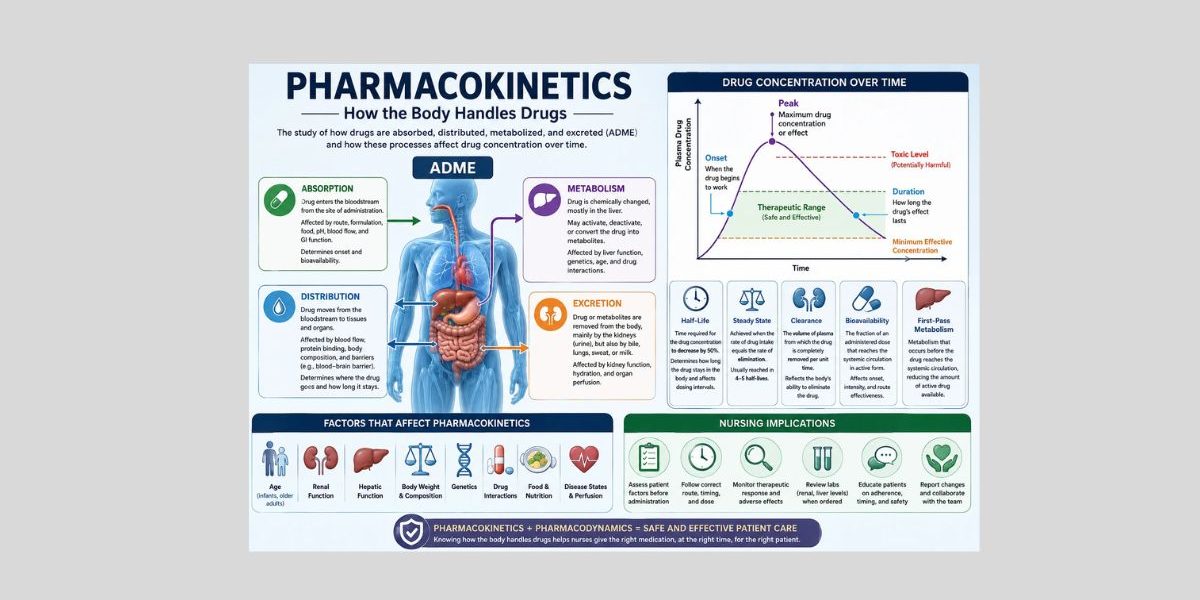
Drug Concentration-Time Curve Explained Simply
A drug concentration-time curve shows how drug concentration changes over time. Students do not need formulas to understand the basic idea.
After administration, drug concentration may rise as absorption occurs. If enough active drug reaches systemic circulation, the concentration may enter the therapeutic range. At some point, the drug may reach a peak concentration or produce a peak effect, depending on the medication and what is being measured. Later, the concentration declines as metabolism and excretion remove the drug from the body.
The curve helps explain three safety zones:
| Zone | Meaning | Nursing relevance |
|---|---|---|
| Subtherapeutic level | Drug level may be too low to produce the intended effect | The patient may not show the expected therapeutic response. |
| Therapeutic range | Drug level is within the desired range for effect and safety | Nurses monitor for expected response and adverse effects. |
| Toxic concentration | Drug level may be high enough to cause harm | Nurses monitor for toxicity signs and report concerns promptly. |
This curve connects many pharmacokinetic concepts. Absorption affects the rising part of the curve. Peak relates to the highest point or strongest useful effect. Metabolism and excretion affect the declining part. Half-life affects how quickly concentration decreases. Repeated dosing affects accumulation and steady state.
In nursing practice, this matters because medication effects happen over time, not instantly in every case. Nurses reassess, monitor, educate, and document based on expected timing, patient condition, ordered monitoring, and facility policy.
Onset, Peak, and Duration of Medication Action
Onset, peak, and duration are core pharmacokinetic concepts for nursing students.
The Onset is when a medication begins to produce an effect.
Peak is when the medication reaches its greatest effect or highest useful concentration, depending on the context.
Duration is how long the medication effect lasts.
Students often confuse onset and peak. Onset is the beginning of an effect. Peak is the strongest or most significant point of effect. A patient may begin to feel relief before the medication reaches peak effect.
| Timeline point | Meaning | Nursing example |
|---|---|---|
| Administration | Medication is given according to order | Nurse verifies patient, medication, dose, route, time, and documentation requirements. |
| Absorption/rising concentration | Drug begins entering circulation or reaching target area | Nurse considers route, formulation, and patient condition. |
| Onset | Drug begins producing an effect | Nurse knows reassessment too early may miss the expected response. |
| Peak | Drug reaches greatest effect or key concentration point | Nurse watches for strongest therapeutic effect and possible adverse effects. |
| Duration | Drug effect continues for a period | Nurse monitors whether symptoms return as effect declines. |
| Decline | Drug level falls as elimination occurs | Nurse observes for subtherapeutic response or need for ordered next dose timing. |
Route, formulation, absorption, metabolism, excretion, patient age, circulation, food, drug interactions, and organ function may all affect onset, peak, and duration.
For example, a medication given orally may need time for gastrointestinal absorption. A transdermal medication may absorb gradually. An IV medication enters circulation directly, but the clinical effect still depends on the drug’s pharmacodynamics, target site, circulation, and patient condition.
Nursing relevance includes timing reassessment, evaluating pain or symptom relief, monitoring for adverse effects, documenting response, and teaching patients not to expect all medications to work immediately.
Onset vs Peak: Key Differences for Nursing Students
| Concept | Meaning | What nurses monitor | Common student mistake | Example |
|---|---|---|---|---|
| Onset | When the medication begins to work | Early therapeutic response | Thinking onset means maximum effect | A patient begins to report some pain relief. |
| Peak | When the medication reaches greatest effect or key concentration point | Strongest response and adverse effects | Reassessing only at onset and missing peak concerns | Sedation or dizziness may be more noticeable near stronger effect. |
| Duration | How long the effect lasts | Return of symptoms or continued response | Assuming duration is the same for every patient | Pain relief may wear off before the next ordered dose for some patients. |
The fastest route or highest concentration depends on medication, formulation, patient condition, circulation, and intended effect. Students should avoid absolute statements such as “IV always works immediately for every clinical effect” or “oral medications always work slowly.” Those statements are too broad.
Half-Life in Pharmacokinetics
Half-life is the time it takes for the amount or concentration of a drug in the body to decrease by half. It helps explain how long drugs remain in the body, how repeated doses may accumulate, and how long it may take to approach steady state (Patel & Barvaliya, 2023).
A short half-life generally means drug concentration decreases faster. A long half-life means the drug remains in the body longer. However, clinical response still depends on the drug, patient factors, active metabolites, and pharmacodynamics.
Half-life matters because repeated doses can accumulate. If a patient receives more medication before the previous amount has been adequately eliminated, drug levels may rise. This can be expected and safe for many medications when ordered correctly, but it can become risky when renal impairment, liver impairment, drug interactions, extra doses, or patient sensitivity affect elimination.
Nursing relevance includes medication timing, missed doses, toxicity risk, patient education, older adult safety, and monitoring of patients with renal or hepatic impairment. Nurses should not calculate or alter dosing intervals independently unless allowed by role, policy, and order. However, nurses should understand why timing instructions and ordered monitoring matter.
A common student mistake is treating half-life as only a math concept. In nursing, half-life is also a safety concept.
Therapeutic Range, Therapeutic Window, and Toxicity
The therapeutic range, sometimes called the therapeutic window, is the range of drug concentration associated with desired effect and acceptable safety for a medication. Below this range, drug levels may be subtherapeutic. Above this range, toxicity risk may increase.
The minimum effective concentration is the level at which a drug begins to produce the intended effect. Toxic concentration refers to a level at which harmful effects may occur. Not every medication requires routine blood-level monitoring, but some medication categories require closer monitoring because the safe and effective range is narrow.
Peak and trough concepts are related to therapeutic monitoring. A peak level refers to a higher concentration point after administration. A trough level refers to a lower concentration point before the next dose. These levels are only collected when ordered and must follow facility timing requirements.
Nursing relevance includes lab monitoring where ordered, observing for adverse effects, recognizing toxicity concerns, documenting patient response, and communicating abnormal findings or clinical changes to the healthcare team.
Students should not confuse therapeutic effect with therapeutic range. Therapeutic effect means the medication is producing the intended clinical response. Therapeutic range refers to a concentration range associated with effectiveness and safety.
Steady State and Drug Accumulation
Steady state occurs when drug intake and drug elimination are balanced during repeated dosing. At this point, the amount of drug entering the body is approximately balanced by the amount being removed.
Steady state usually takes time. Half-life helps explain why. A medication with a longer half-life generally takes longer to approach steady state than one with a shorter half-life.
Drug accumulation happens when drug intake exceeds elimination over time. Accumulation is not always unsafe; it may be expected with regular dosing. However, unexpected accumulation can increase safety risks.
Several factors can affect expected drug levels:
- missed doses
- extra doses
- renal impairment
- liver impairment
- drug interactions
- changes in hydration or perfusion
- altered absorption
- age-related changes
- critical illness
Nursing relevance includes patient education, monitoring delayed effects, watching for adverse effects, and reporting concerns. A patient may not show the full expected effect immediately after starting some medications. Conversely, adverse effects may become more noticeable after repeated doses.
Loading Dose and Maintenance Dose: Basic Concept
A loading dose may be used in some situations to reach a therapeutic level sooner. Maintenance doses help keep drug levels within the desired range over time.
This concept connects to therapeutic range, steady state, half-life, and monitoring. The loading dose is about reaching a useful concentration more quickly. Maintenance dosing is about sustaining the desired concentration.
Nurses should not calculate, adjust, or recommend loading or maintenance doses unless it is within their role, education, policy, and authorized orders. For most nursing students, the goal is conceptual understanding: some medications require strategies to reach and maintain therapeutic levels safely.
Drug Clearance
Clearance is the body’s ability to remove a drug from circulation. It reflects elimination through organs such as the kidneys and liver.
Renal clearance refers to drug removal through the kidneys. Hepatic clearance refers to drug removal through liver metabolism and biliary pathways. Clearance affects drug levels, half-life, accumulation, and toxicity risk.
Clearance may be affected by:
- age
- kidney function
- liver function
- blood flow and perfusion
- hydration
- drug interactions
- critical illness
Nursing relevance is monitoring, not independent dose changing. Nurses may review ordered labs, monitor patient response, assess for adverse effects, observe urine output when relevant, and communicate concerns to prescribers or pharmacists.
A common student mistake is assuming clearance only means urination. Kidney excretion is important, but clearance can involve multiple processes, including hepatic metabolism and biliary elimination.
Patient Factors That Affect Pharmacokinetics
Patients do not process medications identically. Pharmacokinetics can vary based on age, organ function, circulation, body composition, genetics, clinical condition, and interactions.
| Patient factor | Pharmacokinetic effect | Nursing consideration |
|---|---|---|
| Age | Older adults may have changes in body composition, renal function, hepatic function, and protein binding. | Monitor closely for adverse effects and follow ordered parameters. |
| Kidney function | Reduced renal excretion may increase accumulation risk for some drugs. | Review ordered renal labs and report concerns. |
| Liver function | Reduced metabolism may affect active drug levels or metabolite formation. | Watch for adverse effects and liver-related concerns. |
| Pregnancy/lactation | Distribution and exposure considerations may change depending on medication. | Follow provider orders and pregnancy/lactation safety guidance. |
| Body composition | Fat, water, and lean mass may affect distribution. | Consider older adults, obesity, dehydration, and cachexia. |
| Hydration status | Dehydration or fluid overload may affect distribution and renal perfusion. | Monitor intake/output, fluid status, and ordered labs. |
| Albumin/protein levels | Low protein levels may affect free drug levels for highly protein-bound medications. | Watch for stronger effects or adverse effects where relevant. |
| Circulation/perfusion | Poor perfusion can affect absorption, distribution, metabolism, and excretion. | Monitor clinical condition and tissue perfusion indicators. |
| GI function | Vomiting, diarrhea, malabsorption, tube feeding, or delayed gastric emptying may affect absorption. | Verify route, timing, and administration instructions. |
| Genetics | Enzyme differences may affect metabolism for some medications. | Recognize that response can vary among patients. |
| Drug interactions | Interactions may affect absorption, metabolism, protein binding, or excretion. | Perform medication reconciliation and check drug references. |
| Food interactions | Food may increase, decrease, delay, or alter absorption for some drugs. | Teach timing only according to drug reference, order, and policy. |
| Smoking/alcohol/substance use | May affect metabolism, safety, adherence, or organ function. | Assess honestly and nonjudgmentally. |
| Critical illness | Organ perfusion, fluid shifts, inflammation, and organ dysfunction may alter drug movement. | Monitor closely and communicate changes. |
| Adherence/missed doses | Missed or extra doses can affect drug levels and response. | Educate patients and document concerns. |
Route of Administration and Pharmacokinetics
Route of administration affects absorption, onset, bioavailability, and first-pass metabolism.
Oral medications often require gastrointestinal absorption and may be affected by first-pass metabolism. IV medications enter the bloodstream directly and bypass absorption in the usual sense. Sublingual and buccal routes may reduce first-pass effects for certain medications. Transdermal medications usually provide gradual absorption through the skin. Inhaled medications may act locally in the lungs or have systemic effects depending on the drug. Enteral tube administration has special considerations related to formulation, tube type, feeding schedules, and facility policy.
The main point is that route changes are not simple substitutions. Nurses must not change routes without proper authorization. A tablet, liquid, patch, inhaler, injection, or IV form may have different pharmacokinetic behavior even when the medication name seems similar.
This section only summarizes route effects. For a fuller guide, read Medication Administration Routes.
Drug Interactions and Pharmacokinetics
Drug interactions can affect pharmacokinetics by changing absorption, metabolism, protein binding, or excretion.
Food-drug interactions may alter absorption. Some foods may delay absorption, reduce absorption, increase absorption, or irritate the gastrointestinal tract depending on the medication.
Drug-drug interactions may affect metabolism. Enzyme inhibition can reduce metabolism of some medications, potentially increasing drug levels. Enzyme induction can increase metabolism of some medications, potentially reducing exposure. This is a simplified explanation, but it helps students understand why medication reconciliation matters.
Interactions may also affect renal excretion or protein binding. If two medications compete for similar pathways, drug levels or effects may change.
Nursing relevance includes medication reconciliation, asking about over-the-counter drugs and supplements according to policy, checking drug references, teaching patients to follow medication instructions, and reporting concerns. Students should avoid giving independent management advice. The nurse’s role is to identify risks, monitor, educate within scope, and communicate.
Nursing Responsibilities in Pharmacokinetics
Nurses use pharmacokinetic thinking before, during, and after medication administration.
Key responsibilities include:
- verifying the medication order, route, timing, patient identity, and documentation requirements
- assessing allergies and contraindication concerns according to policy
- reviewing relevant labs where ordered
- considering kidney function and liver function
- assessing patient factors such as age, swallowing ability, GI status, hydration, perfusion, and mental status
- monitoring therapeutic response
- monitoring adverse effects and toxicity signs
- reassessing at appropriate times based on expected onset, peak, and duration
- educating patients about timing, missed doses, food interactions, and safety where appropriate
- documenting medication administration and patient response
- communicating concerns to the healthcare team
Nurses are often the final safety checkpoint before medication reaches the patient. Medication administration safety literature emphasizes that nurses play a central role in checking, administering, monitoring, and communicating medication-related concerns (Hanson & Haddad, 2023; Hughes & Blegen, 2008).
Pharmacokinetics helps nurses ask better questions. Is this medication expected to work quickly or gradually? Does this patient have renal impairment? Should the patient be reassessed near the expected peak? Are there signs of toxicity? Has the patient missed doses? Are labs ordered? Does the route match the order?
These questions turn pharmacology into clinical reasoning.
Pharmacokinetics and Medication Safety
Pharmacokinetics supports medication safety because timing, route, organ function, and drug concentration matter.
Timing matters because a medication may not produce an immediate effect. If nurses reassess too soon, they may assume the drug failed. If they reassess too late, they may miss adverse effects or inadequate response.
Route matters because different routes can change absorption, bioavailability, onset, and first-pass metabolism. A route error can create safety risks.
Duplicate doses can be risky because repeated exposure may increase drug levels, especially when half-life is long or clearance is reduced.
Renal and liver impairment can increase medication risk because elimination may be slowed. Therapeutic range matters because some medications have a narrower margin between effective and toxic levels.
Monitoring matters because the same medication category can affect patients differently. Pharmacokinetics teaches students that medication safety is not only about memorizing drug names. It is about understanding how patient factors and drug movement affect response.
Common Pharmacokinetics Mistakes Students Make
Confusing pharmacokinetics with pharmacodynamics
Pharmacokinetics is drug movement through the body. Pharmacodynamics is drug action on the body.
Memorizing ADME without clinical meaning
ADME is not just vocabulary. It explains timing, route effects, monitoring, organ function, and safety.
Confusing onset with peak
Onset is when the drug begins to work. Peak is when the effect or concentration is greatest.
Assuming IV always means immediate clinical effect
IV administration places medication directly into circulation, but the clinical effect still depends on the drug, target site, circulation, and pharmacodynamics.
Ignoring half-life
Half-life affects duration, accumulation, steady state, missed doses, and toxicity risk.
Ignoring renal or liver function
Kidney and liver function can strongly affect drug elimination and safety.
Assuming all oral drugs absorb the same way
Oral absorption varies by drug, formulation, food, GI function, and first-pass metabolism.
Forgetting first-pass metabolism
Some orally administered drugs lose active concentration before reaching systemic circulation.
Confusing therapeutic effect with therapeutic range
Therapeutic effect is the desired clinical response. Therapeutic range is a drug concentration range associated with effect and safety.
Assuming nurses can change routes or doses independently
Nurses must follow provider orders, facility policy, drug references, supervision requirements, and scope of practice.
Using drug names without understanding the concept
Students may list medications in assignments without explaining absorption, metabolism, excretion, half-life, or monitoring relevance.
Pharmacokinetics in Nursing Assignments
Pharmacokinetics appears in many nursing assignments. Students may need to explain how medication movement affects care planning, patient monitoring, safety, and documentation.
| Assignment type | How to discuss pharmacokinetics | Example focus |
|---|---|---|
| Pharmacology assignment | Explain ADME, half-life, onset, peak, and monitoring. | How renal function affects medication safety. |
| Medication case study | Connect patient factors to medication response. | Older adult with reduced kidney function and adverse-effect risk. |
| Nursing care plan | Link medication monitoring to nursing interventions. | Monitor therapeutic response and adverse effects after administration. |
| SOAP note | Include medication response in subjective/objective data and plan. | Patient reports pain relief after medication; nurse monitors sedation. |
| Clinical reflection | Reflect on how timing and reassessment affected care. | Reassessing at the expected onset and documenting response. |
| Patient education assignment | Explain safe medication timing and missed-dose instructions based on approved guidance. | Teaching the patient not to double doses unless instructed by a provider. |
| Research paper | Discuss pharmacokinetic concepts using scholarly sources. | Bioavailability, first-pass metabolism, and route effects. |
| Discussion post | Compare concepts briefly and apply them to nursing practice. | Pharmacokinetics vs pharmacodynamics in medication monitoring. |
If you are writing a pharmacology paper, case study, or care plan, you may also find these academic support pages useful: nursing assignment help, nursing coursework help, nursing case study help, and nursing research paper help.
Keep the writing clinical and specific. Do not simply define ADME. Explain why ADME matters for patient monitoring and safety.
Pharmacokinetics Essay and Study Topics
Useful pharmacokinetics topics include:
- pharmacokinetics vs pharmacodynamics
- ADME in nursing pharmacology
- half-life and medication safety
- onset vs peak in medication monitoring
- bioavailability and first-pass metabolism
- renal function and drug excretion
- liver metabolism and medication response
- route of administration and absorption
- pharmacokinetics in older adults
- therapeutic range and toxicity
- drug interactions and pharmacokinetics
- nursing responsibilities in medication monitoring
Students should narrow broad topics by medication category, patient population, pharmacokinetic concept, safety issue, or nursing responsibility.
For example, “pharmacokinetics in nursing” is too broad for many essays. A stronger topic might focus on how renal impairment affects drug excretion and nursing monitoring in older adults.
Sample Thesis Statement and Paragraph Structure
Sample thesis statement:
“Pharmacokinetics is important in nursing because it helps nurses understand how drugs are absorbed, distributed, metabolized, and excreted, allowing safer monitoring of onset, peak effect, duration, therapeutic response, and toxicity risk.”
A strong paragraph structure can follow this pattern:
- Topic sentence
- Define the pharmacokinetic concept
- Explain how it affects medication action or safety
- Give a nursing example
- Explain the nursing responsibility or monitoring implication
Example paragraph approach:
Start by naming the concept, such as half-life. Define it in simple terms. Then explain why it matters for accumulation, duration, and monitoring. Add a nursing example, such as watching for adverse effects in a patient with reduced renal function. End by explaining the nurse’s role in reassessment, documentation, and communication.
Quick Pharmacokinetics Checklist for Nursing Students
Use this checklist before exams, care plans, case studies, or pharmacology assignments:
- Can I define pharmacokinetics?
- Can I explain ADME?
- Can I distinguish pharmacokinetics from pharmacodynamics?
- Do I know what absorption means?
- Do I understand bioavailability and first-pass metabolism?
- Can I explain distribution, metabolism, and excretion?
- Can I tell the difference between onset, peak, and duration?
- Do I understand half-life at a conceptual level?
- Can I explain therapeutic range and toxicity risk?
- Can I identify patient factors that affect pharmacokinetics?
- Can I connect the concept to nursing monitoring and patient safety?
FAQs About Pharmacokinetics
What is pharmacokinetics in simple terms?
Pharmacokinetics means what the body does to a drug. It explains how the body absorbs, distributes, metabolizes, and excretes medication.
What are the four stages of pharmacokinetics?
The four stages are absorption, distribution, metabolism, and excretion. These are often abbreviated as ADME.
What is the difference between pharmacokinetics and pharmacodynamics?
Pharmacokinetics explains how the body moves and processes a drug. Pharmacodynamics explains what the drug does to the body, including therapeutic effects, side effects, adverse effects, and toxicity.
What does ADME mean in pharmacokinetics?
ADME stands for absorption, distribution, metabolism, and excretion. It helps students organize how a drug enters the body, moves through tissues, changes chemically, and leaves the body.
What is the difference between onset and peak?
Onset is when a medication begins to produce an effect. Peak is when the medication reaches its greatest effect or important concentration point.
Why is half-life important in nursing?
Half-life helps nurses understand how long a drug may remain in the body, how repeated doses can accumulate, and why timing and monitoring matter.
How do kidney and liver function affect pharmacokinetics?
The kidneys help excrete many drugs and metabolites. The liver helps metabolize many drugs. Reduced kidney or liver function can affect drug levels, duration, accumulation, and toxicity risk.
Why do nursing students need to understand pharmacokinetics?
Nursing students need pharmacokinetics because it connects medication administration to clinical reasoning. It helps them understand timing, monitoring, route effects, adverse effects, therapeutic response, and patient safety.
Final Thoughts on Pharmacokinetics
Pharmacokinetics helps nursing students understand how drugs move through the body. It explains why medication timing matters, how onset and peak differ, how half-life and clearance affect monitoring, and why patient factors influence medication safety.
The main lesson is simple: do not treat pharmacokinetics as memorized vocabulary. Use it as a clinical reasoning tool.
When students understand ADME, bioavailability, first-pass metabolism, half-life, therapeutic range, steady state, clearance, and patient factors, they can write stronger assignments and think more safely in clinical settings.
If students need help writing a pharmacokinetics essay, pharmacology assignment, nursing case study, SOAP note, care plan, discussion post, or research paper, they can upload their instructions and request academic guidance.
References
Alagga, A. A., & Gupta, V. (2024). Drug absorption. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557405/
Ernstmeyer, K., & Christman, E. (2023). Nursing pharmacology: Pharmacokinetics and pharmacodynamics. Open RN/NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK595006/
Garza, A. Z., Park, S. B., & Kocz, R. (2023). Drug elimination. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK547662/
Hanson, A., & Haddad, L. M. (2023). Nursing rights of medication administration. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK560654/
Herman, T. F., & Santos, C. (2023). First pass effect. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK551679/
Hughes, R. G., & Blegen, M. A. (2008). Medication administration safety. In R. G. Hughes (Ed.), Patient safety and quality: An evidence-based handbook for nurses. Agency for Healthcare Research and Quality. https://www.ncbi.nlm.nih.gov/books/NBK2656/
Onetto, A. J., & Sharif, S. (2023). Drug distribution. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK567736/
Patel, K., & Barvaliya, M. (2023). Pharmacokinetics. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557744/
Price, G., & Patel, D. A. (2023). Drug bioavailability. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557852/
Susa, S. T., Hussain, A., & Preuss, C. V. (2023). Drug metabolism. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK442023/