Cardiac medications are drugs used to support heart and blood vessel conditions, but nursing students must understand more than medication names. These medications can affect blood pressure, pulse, heart rhythm, clotting, cholesterol, fluid balance, renal function, electrolytes, fall risk, and patient safety.
Many students memorize common cardiac medications but struggle to connect them with real nursing decisions. For example, a student may remember that beta blockers can affect heart rate, but still miss the importance of checking the pulse trend, reviewing the blood pressure, listening to the patient’s symptoms, checking the medication order, and asking for guidance before administration when something seems unsafe.
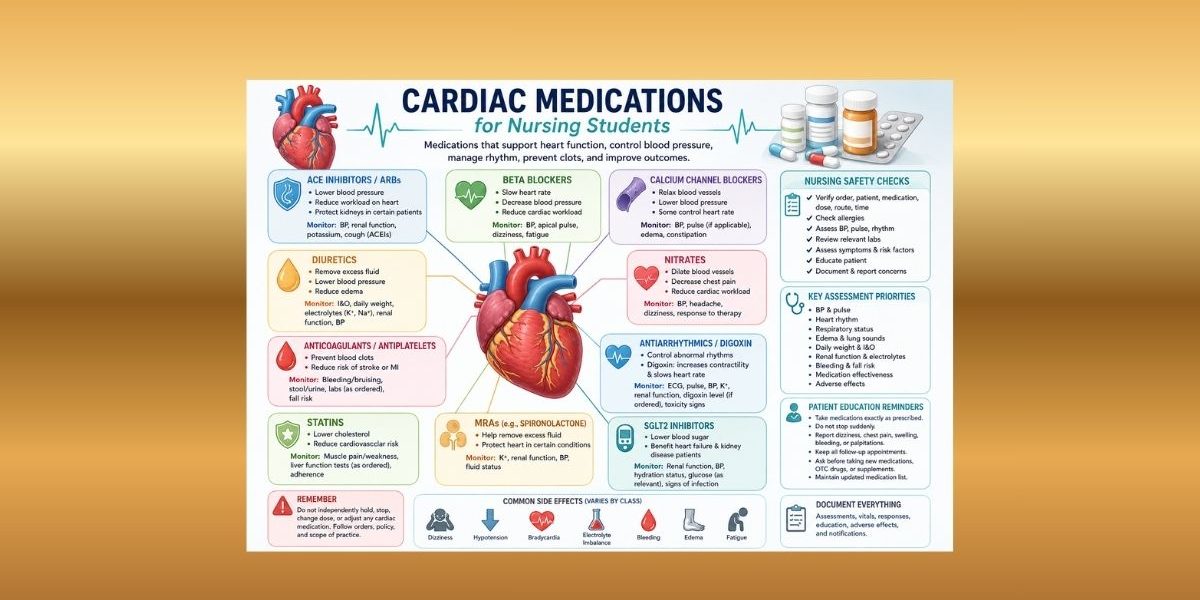
This guide explains major classes of cardiac medications, common examples, nursing responsibilities, monitoring priorities, adverse effects, patient education, documentation, clinical judgment, and scope-of-practice boundaries. It is designed for nursing students, pre-nursing students, ADN students, BSN students, RN-to-BSN students, pharmacology students, cardiac nursing students, clinical skills students, and healthcare students preparing for clinical practice.
This guide is for nursing education and pharmacology learning only. Cardiac medication use must follow provider orders, medication labels, approved drug references, facility policy, pharmacist guidance, instructor guidance, and scope of practice.
Quick Answer: What Are Cardiac Medications?
- Cardiac medications are drugs used to support heart and blood vessel conditions when clinically appropriate and ordered.
- They may affect blood pressure, heart rate, rhythm, contractility, fluid balance, clotting, cholesterol, or cardiac workload.
- Common classes include beta blockers, ACE inhibitors, ARBs, ARNIs, calcium channel blockers, diuretics, nitrates, anticoagulants, antiplatelets, antiarrhythmics, cardiac glycosides, statins, SGLT2 inhibitors, and mineralocorticoid receptor antagonists.
- Nurses do not independently choose, dose, hold, titrate, restart, or adjust cardiac medications unless following provider orders and facility policy.
- Nursing responsibilities include order verification, vital sign monitoring, rhythm awareness, lab review where assigned, adverse-effect monitoring, patient education, communication, and documentation.
- Cardiac medications require careful safety checks because they can affect blood pressure, pulse, rhythm, electrolytes, kidney function, bleeding risk, and fall risk.
What Are Cardiac Medications in Nursing?
Cardiac medications are ordered pharmacologic therapies used in cardiovascular care. They may be used in patients with high blood pressure, heart failure, coronary artery disease, arrhythmias, clotting risk, fluid overload, cholesterol concerns, or other cardiovascular conditions. The American Heart Association identifies several cardiovascular medication categories, including ACE inhibitors, ARBs, beta blockers, calcium channel blockers, diuretics, nitrates, anticoagulants, antiplatelets, and cholesterol-lowering medications (American Heart Association, 2025a).
In nursing, understanding cardiac medications does not mean learning how to prescribe them. Nursing students study cardiac medications so they can safely administer ordered medications, recognize assessment priorities, monitor therapeutic response, identify possible adverse effects, educate patients within scope, and document care accurately.
A nurse’s role is practical and safety-focused. Before administering an ordered cardiac medication, the nurse may need to verify the order, check patient identity, review allergies, assess blood pressure, assess pulse, consider rhythm context, review relevant labs, evaluate symptoms, consider fall risk, and follow facility policy. The exact nursing responsibilities depend on the medication, setting, patient condition, order, and scope of practice.
For example, a medication that lowers blood pressure should not be viewed only as “a blood pressure drug.” The student should think:
- What is the patient’s baseline blood pressure?
- What is the current blood pressure?
- Is the patient dizzy, weak, short of breath, or unsteady?
- Does the medication also affect pulse or rhythm?
- Are there relevant labs?
- Is the order clear?
- Does facility policy require a specific check before administration?
- Should I ask the RN, instructor, pharmacist, provider, or preceptor for guidance?
That connection between medication action and patient assessment is the foundation of safe cardiac medications nursing practice.
Why Nursing Students Need to Understand Cardiac Medications
Cardiac medications are common in adult health, medical-surgical nursing, older adult care, community health, chronic disease management, cardiac units, emergency settings, rehabilitation, and high-acuity care. Students may see them in clinical rotations, simulation labs, case studies, medication cards, care plans, and pharmacology exams.
These medications matter because they can change the same findings nurses assess every day. A beta blocker may affect pulse and blood pressure. A diuretic may affect fluid balance, weight, urine output, and electrolytes. An anticoagulant may increase bleeding-risk concerns. A statin may require patient education about muscle symptoms and adherence. Digoxin may require attention to pulse, renal function, potassium, toxicity symptoms, and ordered serum levels.
Medication safety depends on more than memorizing a cardiac medications list. A student must learn how to connect the drug class to the patient’s condition. The question is not only, “What does this medication do?” A stronger nursing question is, “What should I assess before and after this medication, and what findings would require clarification or reporting?”
Nurses often notice changes early because they spend time assessing patients, reviewing trends, administering medications, answering patient questions, and documenting responses. A patient may say, “I feel lightheaded when I stand,” “My heart feels slow,” “My legs look more swollen,” “My gums are bleeding,” or “I stopped taking that medication because I felt tired.” These statements can become important clinical cues.
Students who understand cardiac medications can better organize care plans, medication cards, patient education plans, clinical reflections, and case study answers. They also become safer in clinical practice because they learn to pause, assess, clarify, and report instead of guessing.
How Cardiac Medications Affect the Body
Cardiac medications can affect the cardiovascular system in different ways. Some reduce blood pressure, while some slow the heart rate. Others influence clot formation. Some reduce cholesterol. Some affect fluid balance. Others help selected patients with heart failure or rhythm-related conditions.
This is where students should connect pharmacodynamics for nursing students with bedside assessment. Pharmacodynamics explains what the medication does to the body, while nursing assessment helps determine how the patient is responding.
| Medication effect | What it may change | Nursing assessment connection |
|---|---|---|
| Lowers blood pressure | Vascular tone, cardiac workload, or fluid volume | Blood pressure trends, dizziness, weakness, falls risk, orthostatic symptoms |
| Slows heart rate | Cardiac rate or conduction | Pulse, apical pulse where required, rhythm context, fatigue, dizziness |
| Changes fluid balance | Sodium/water excretion or retention | Intake/output, edema, lung sounds, daily weight, dehydration signs |
| Affects clotting | Platelet activity or coagulation pathways | Bleeding, bruising, stool/urine changes, fall risk, ordered labs |
| Affects electrolytes | Potassium, sodium, magnesium, calcium | Rhythm safety, weakness, lab reporting, renal context |
| Affects renal workload or clearance | Kidney function and medication handling | Creatinine/eGFR trends where ordered, urine output, dose-safety awareness |
| Affects cholesterol | Lipid levels and cardiovascular risk | Adherence education, lipid panels where ordered, muscle symptom reporting |
| Affects cardiac workload | Oxygen demand, rate, pressure, or contractility | Chest discomfort reports, fatigue, blood pressure, pulse, symptom response |
Students should also understand pharmacokinetics for nursing students because renal clearance, metabolism, half-life, serum levels, and drug accumulation may affect cardiac medication safety. This is especially relevant when reviewing renal function, electrolyte trends, and ordered drug levels.
Cardiac Medications and Nursing Safety Checks
Safe cardiac medication administration begins before the medication is given. Medication administration safety sources emphasize the importance of checking the right patient, medication, dose, route, time, and documentation. Nurses are often the final checkpoint before administration, which makes assessment and verification essential (Hanson & Haddad, 2023).
| Safety check | Why it matters | Nursing student focus |
|---|---|---|
| Patient identity | Prevents wrong-patient medication errors | Use facility-approved identifiers before administration. |
| Medication order and MAR | Confirms what was ordered and scheduled | Compare medication name, dose, route, time, frequency, and order status. |
| Allergies | Reduces risk of allergic or adverse reactions | Check allergy history and clarify unclear reactions. |
| Medication label | Prevents wrong-medication and wrong-strength errors | Compare label with MAR according to policy. |
| Route | Cardiac medications may be oral, IV, transdermal, sublingual, or other ordered routes | Follow order, route-specific policy, and instructor guidance. |
| Blood pressure | Many cardiac medications affect vascular tone, workload, or fluid status | Review baseline, current reading, trend, and symptoms. |
| Apical/radial pulse | Some medications affect rate or rhythm | Assess pulse as required by order, policy, drug reference, or instructor guidance. |
| Heart rhythm/ECG context | Some medications are used in rhythm-related care | Know whether telemetry or rhythm monitoring is ordered or assigned. |
| Respiratory status and oxygen saturation | Cardiac and respiratory symptoms can overlap | Assess shortness of breath, oxygen saturation, and lung sounds where relevant. |
| Renal function | Some cardiac medications affect or depend on kidney function | Review ordered labs according to scope and report concerns. |
| Electrolytes | Potassium, sodium, magnesium, and calcium may affect cardiac safety | Connect electrolytes to diuretics, rhythm risk, digoxin, and renal context. |
| Bleeding risk | Anticoagulants and antiplatelets require bleeding awareness | Watch for bruising, bleeding, stool/urine changes, and fall risk. |
| Fall/orthostatic risk | Hypotension and dizziness can cause injury | Assess dizziness, weakness, gait, and posture-related symptoms. |
| Fluid balance | Diuretics and heart failure medications may affect volume status | Track intake/output, edema, lung sounds, and daily weight where ordered. |
| Patient understanding | Misunderstanding can lead to unsafe use | Reinforce provider/pharmacist instructions and ask what the patient understands. |
| Documentation | Creates a legal and clinical record | Document administration, assessments, patient response, education, and notifications. |
Students should also review medication administration routes because cardiac medications may be ordered by different routes, including oral, sublingual, transdermal, or IV routes depending on the setting, medication, order, and facility policy.
Classes of Cardiac Medications
The classes of cardiac medications help nursing students organize what to monitor. A class-based approach is safer than trying to memorize hundreds of medication names without understanding the expected effects.
| Class | General purpose | Common nursing monitoring focus | Important caution |
|---|---|---|---|
| Beta blockers | Reduce heart rate, blood pressure, and cardiac workload | Pulse, BP, dizziness, fatigue, respiratory symptoms where relevant | Avoid universal hold parameters. Follow order and policy. |
| ACE inhibitors | Support blood pressure and selected cardiac/renal contexts | BP, renal function, potassium, cough, angioedema awareness | Do not independently substitute or adjust therapy. |
| ARBs | Support blood pressure and selected cardiac/renal contexts | BP, renal function, potassium, dizziness | Avoid assuming they are identical to ACE inhibitors. |
| ARNIs | Used in selected heart failure contexts | BP, renal function, potassium, fluid symptoms | Keep details aligned with current guidelines and course materials. |
| Calcium channel blockers | Affect vascular tone, BP, and sometimes heart rate | BP, pulse where relevant, edema, dizziness, constipation | Medications in the class differ. |
| Diuretics | Support fluid removal or fluid balance | I&O, daily weight, edema, lung sounds, electrolytes, renal function | Do not independently adjust dose or potassium replacement. |
| Nitrates | Reduce cardiac workload or improve blood flow depending on context | BP, headache, dizziness, orthostatic symptoms, symptom response | Do not turn into a chest pain protocol. |
| Anticoagulants | Reduce clot formation risk where ordered | Bleeding signs, bruising, ordered labs, fall risk, interactions | Avoid reversal-agent or INR adjustment instructions. |
| Antiplatelets | Reduce platelet-related clotting risk where ordered | Bleeding, bruising, medication history, education | Do not manage therapy independently. |
| Antiarrhythmics | Support rhythm management when ordered | ECG/rhythm context, pulse, BP, ordered labs | Do not teach rhythm-management algorithms. |
| Cardiac glycosides | Affect contractility and rate-related concepts | Pulse, renal function, potassium, toxicity awareness, ordered levels | Digoxin requires careful monitoring but no universal hold rule here. |
| Statins | Lower cholesterol and support cardiovascular risk reduction | Muscle symptoms, liver-related labs where ordered, adherence | Do not provide individualized cholesterol treatment advice. |
| SGLT2 inhibitors | Used in selected cardiac, renal, and endocrine contexts | Volume status, renal function, glucose context, education | Do not provide prescribing criteria or dosing guidance. |
| Mineralocorticoid receptor antagonists | Used in selected cardiac contexts | Potassium, renal function, BP, fluid status | Do not provide patient-selection or dosing rules. |
| Vasodilators | Relax blood vessels in selected ordered contexts | BP, dizziness, headache, response | Avoid treatment algorithms. |
This article introduces cardiac medication classes broadly. Classes of Cardiac Medications article goes deeper into mechanisms, examples, and study tables.
Beta Blockers: Nursing Considerations
Beta blockers may be used in cardiovascular care to reduce heart rate, reduce blood pressure, decrease cardiac workload, support selected rhythm contexts, or support care after certain cardiac events when ordered. The American Heart Association describes beta blockers as medications that can prevent the heart from beating too quickly and forcefully (American Heart Association, 2025b).
Nursing students should associate beta blockers with pulse, blood pressure, activity tolerance, dizziness, fatigue, and symptom trends. The assessment should not stop at one number. A low pulse matters more when paired with symptoms such as dizziness, weakness, shortness of breath, chest discomfort, or unusual fatigue.
Students should avoid saying, “Hold all beta blockers if the pulse is below a certain number.” That kind of universal statement is unsafe because medication orders, patient conditions, facility policies, and clinical contexts differ. The safer nursing approach is to assess, verify the order, compare the finding with facility policy, and ask for guidance when needed.
Patient education may include taking the medication as prescribed, not stopping suddenly unless instructed by the provider, reporting dizziness or fainting, and following blood pressure or pulse monitoring instructions if ordered. The nurse should reinforce provider and pharmacist instructions rather than creating independent medication rules.
ACE Inhibitors and ARBs: Nursing Considerations
ACE inhibitors and ARBs are commonly discussed as blood pressure medications and may appear in cardiovascular, renal, and heart failure contexts. They can help relax blood vessels and reduce cardiac workload when clinically appropriate and ordered (American Heart Association, 2025a).
Nursing students should monitor blood pressure, dizziness, renal function, potassium, and patient symptoms. ACE inhibitors may be associated with cough in some patients, and angioedema awareness is important as a safety concept. ARBs are related but distinct medications, so students should not assume that one medication can be substituted for another without a provider order.
The nursing reasoning is straightforward: these medications can affect blood pressure and renal/electrolyte context, so students should connect vital signs and ordered labs with symptoms. A patient who reports lightheadedness after starting a blood pressure medication needs assessment and reporting according to policy. A potassium or renal function concern should be escalated according to scope and facility process.
Students should not provide treatment advice, dose adjustment, or medication-substitution guidance. Use approved references, facility policy, pharmacist guidance, and provider orders.
ARNIs and Modern Heart Failure Medication Concepts
ARNIs, or angiotensin receptor-neprilysin inhibitors, may appear in modern heart failure pharmacology education. Current heart failure guideline education includes several medication categories used in selected heart failure care, including ARNIs, beta blockers, mineralocorticoid receptor antagonists, and SGLT2 inhibitors (Heidenreich et al., 2022).
For nursing students, the purpose is not to memorize a heart failure prescribing sequence. The purpose is to understand what must be monitored: blood pressure, renal function, potassium, fluid status, dizziness, adherence, and patient symptoms.
Because heart failure medication concepts change as evidence evolves, students should confirm details with current course materials, approved drug references, guideline resources, facility policy, pharmacists, instructors, and providers.
Calcium Channel Blockers: Nursing Considerations
Calcium channel blockers may affect vascular tone, blood pressure, and sometimes heart rate depending on the medication. Students should avoid treating all calcium channel blockers as identical. Some are more closely associated with vascular effects, while others may have more rate-related relevance in selected contexts.
Nursing monitoring may include blood pressure, pulse where relevant, dizziness, edema, constipation where relevant, and therapeutic response. A student should also observe how the patient feels. For example, new dizziness, swelling, weakness, or unusually low blood pressure may require reassessment and reporting.
Patient education should stay general and safe. Reinforce taking the medication as prescribed, reporting dizziness or swelling as instructed, and asking a pharmacist or provider before adding new medications or supplements. Do not provide dosing, hold parameters, or treatment decisions.
Diuretics: Nursing Considerations
Diuretics may be used in contexts involving fluid balance, edema, blood pressure, or cardiac workload. Nursing students should connect diuretics with intake and output, urine output, daily weight where ordered, edema, lung sounds where relevant, blood pressure, renal function, dehydration signs, electrolyte trends, and fall risk.
Diuretics are a strong example of why medication knowledge and assessment must work together. A patient may have less edema and improved breathing, which may suggest a therapeutic response. Another patient may become dizzy, weak, dehydrated, or show electrolyte changes, which may suggest a safety concern.
Potassium deserves special attention, but students should avoid oversimplifying it. Some diuretics may contribute to potassium loss, while others may increase potassium risk. The nurse should review ordered labs according to scope and report concerns, but should not independently decide potassium replacement, medication dose changes, or medication discontinuation.
Patient education may include following ordered weight monitoring, reporting dizziness or severe weakness, following diet or fluid instructions given by the provider, and attending ordered lab appointments. Documentation should include relevant fluid-balance findings, vital signs, response, education, and communication.
Nitrates and Vasodilators: Nursing Considerations
Nitrates and vasodilators may reduce cardiac workload or improve blood flow depending on the order and clinical context. Nitrate-related nursing concerns include blood pressure changes, headache, dizziness, orthostatic symptoms, and symptom response. StatPearls describes nitrates as medications used for cardiovascular conditions, with hypotension and headache among important adverse-effect considerations (Lee & Gerriets, 2023).
This section is not a chest pain protocol. Nursing students should not use it to make emergency decisions, provide dosing instructions, or teach independent treatment steps. Instead, students should understand that symptom changes, low blood pressure, severe dizziness, or worsening discomfort require prompt reporting according to policy and patient condition.
Patient education should reinforce provider instructions, safe use as prescribed, and reporting concerning symptoms. Documentation should include assessment findings, symptoms, medication administration details, patient response, and notifications where required.
Anticoagulants and Antiplatelets: Nursing Considerations
Anticoagulants and antiplatelets are often called “blood thinners,” but they do not literally thin the blood. They reduce clot formation risk through different mechanisms. MedlinePlus explains that anticoagulants and antiplatelet drugs help prevent clots from forming and that bleeding is an important safety concern (MedlinePlus, 2024).
Nursing monitoring focuses on bleeding risk, bruising, bleeding gums, nosebleeds, blood in urine or stool, heavy or prolonged bleeding, fall risk, medication interactions according to approved references, and ordered labs. Students should also ask about patient understanding because anticoagulant and antiplatelet safety often depends on education, adherence, and prompt reporting.
Patient education may include reporting bleeding concerns, using an updated medication list, asking a pharmacist or provider before taking new OTC medications or supplements, avoiding medication sharing, and following lab or follow-up instructions where ordered. Students should not create independent rules about stopping the medication before procedures or changing doses.
Avoid anticoagulation protocols in this article. Do not list reversal agents, INR adjustment rules, bridging protocols, perioperative hold instructions, or protocol-based dose changes. The nursing role is assessment, safety monitoring, communication, education, and documentation within policy and scope.
Antiarrhythmics: Nursing Considerations
Antiarrhythmics are medications used for rhythm management when ordered. They differ widely, so nursing students should not treat the class as one simple group. Some antiarrhythmics require careful rhythm awareness, pulse and blood pressure monitoring, adverse-effect assessment, and ordered lab review.
Students should understand why ECG or rhythm context matters. A rhythm-related medication is not just another pill on the MAR. It may connect to telemetry, pulse changes, dizziness, palpitations, faintness, blood pressure changes, and provider-specific monitoring instructions.
However, students should not learn antiarrhythmics as treatment algorithms. Do not decide how to manage a rhythm, change a dose, or select a medication. If a patient reports palpitations, dizziness, fainting, chest discomfort, or new weakness, the student should reassess within role, notify the RN or instructor, follow facility policy, and document clearly.
Cardiac Glycosides and Digoxin Nursing Implications
Digoxin is a common nursing-school example because it connects pulse assessment, renal function, potassium context, toxicity awareness, ordered serum levels, and patient education. StatPearls describes digoxin as a cardiac glycoside with positive inotropic effects and AV-node effects, and it highlights the need for careful safety awareness due to toxicity risk (David & Shetty, 2024).
For nursing students, digoxin nursing implications should stay focused on assessment and reporting. Students should understand why pulse checks may be required, why potassium and renal function matter, why ordered levels may be monitored, and why symptoms such as unusual weakness, nausea, confusion, visual changes, dizziness, or rhythm concerns may need reporting.
Do not give universal pulse hold parameters. Also, do not provide digoxin dosing. Avoid teaching toxicity treatment steps. Do not interpret serum levels as a standalone rule. Digoxin safety depends on the full patient picture, provider orders, facility policy, approved references, and clinical supervision.
A future Digoxin Nursing Implications article can go deeper into nursing-school learning points while still avoiding unsafe prescribing or treatment instructions.
Statins and Cholesterol-Lowering Medications
Statins are cholesterol-lowering medications used in cardiovascular risk reduction contexts when ordered. StatPearls explains that statins are HMG-CoA reductase inhibitors used to lower lipid levels, with examples including atorvastatin, rosuvastatin, simvastatin, pravastatin, fluvastatin, lovastatin, and pitavastatin (Sizar et al., 2024).
Nursing considerations include medication adherence, patient education, muscle symptom reporting, liver-related labs where ordered, lipid panels where ordered, and interaction awareness according to approved references. A student should not provide individualized cholesterol treatment advice or tell a patient which statin is best.
Patient education may include taking the medication as prescribed, reporting new or severe muscle symptoms according to provider instructions, keeping follow-up appointments, and asking a pharmacist or provider before adding new medications or supplements.
SGLT2 Inhibitors and Cardiac Care
SGLT2 inhibitors may appear in modern cardiac and heart failure education, although they also have endocrine and renal relevance. The 2022 AHA/ACC/HFSA heart failure guideline includes SGLT2 inhibitors among contemporary medication classes used in selected heart failure contexts (Heidenreich et al., 2022).
At the nursing-student level, monitoring concepts may include volume status, renal function, glucose context where relevant, hydration concerns, patient education, and adverse-effect awareness according to approved references. Students should understand that a medication can belong to more than one learning category. SGLT2 inhibitors may appear in diabetes, renal, and cardiac discussions.
Do not provide prescribing criteria, dosing guidance, or treatment algorithms. This pillar article introduces the concept only because it is relevant to modern cardiac pharmacology education.
Mineralocorticoid Receptor Antagonists
Mineralocorticoid receptor antagonists may be used in selected cardiac contexts when ordered. They are important in nursing pharmacology because they connect cardiac medications with potassium, renal function, blood pressure, and fluid status. The 2022 AHA/ACC/HFSA heart failure guideline includes mineralocorticoid receptor antagonists among medication categories used in selected heart failure care (Heidenreich et al., 2022).
Nursing students should monitor potassium, renal function, blood pressure, edema, daily weight where ordered, and patient symptoms. The student’s role is not to decide eligibility, dose, or treatment sequence. The role is to recognize why labs and symptoms matter, report concerns, and document appropriately.
Common Cardiac Medications Students Should Recognize
This section gives a short recognition-oriented overview. It is not a complete cardiac medications list. Common Cardiac Medications article can provide a more complete reference.
| Class | Common example names | Nursing monitoring focus |
|---|---|---|
| Beta blockers | Metoprolol, atenolol, carvedilol, propranolol | Pulse, BP, dizziness, fatigue, symptoms |
| ACE inhibitors | Lisinopril, enalapril, captopril | BP, renal function, potassium, cough, angioedema awareness |
| ARBs | Losartan, valsartan, candesartan | BP, renal function, potassium, dizziness |
| ARNIs | Sacubitril/valsartan | BP, renal function, potassium, fluid status |
| Calcium channel blockers | Amlodipine, diltiazem, verapamil | BP, pulse where relevant, edema, dizziness, constipation |
| Diuretics | Furosemide, hydrochlorothiazide, spironolactone | I&O, daily weight, electrolytes, renal function, BP |
| Nitrates | Nitroglycerin, isosorbide mononitrate | BP, headache, dizziness, symptom response |
| Anticoagulants | Warfarin, heparin, enoxaparin, apixaban, rivaroxaban | Bleeding, bruising, ordered labs, fall risk |
| Antiplatelets | Aspirin, clopidogrel | Bleeding, bruising, patient education, medication history |
| Antiarrhythmics | Amiodarone, sotalol, flecainide | Rhythm context, pulse, BP, ordered labs, adverse effects |
| Cardiac glycosides | Digoxin | Pulse, potassium, renal function, toxicity awareness, ordered levels |
| Statins | Atorvastatin, rosuvastatin, simvastatin | Muscle symptoms, lipid panels, liver-related labs where ordered |
| SGLT2 inhibitors | Empagliflozin, dapagliflozin | Volume status, renal function, glucose context, education |
| MRAs | Spironolactone, eplerenone | Potassium, renal function, BP, fluid status |
Cardiac Medications Cheat Sheet for Nursing Students
This brief cardiac medications cheat sheet summarizes the key nursing connection for each major class. It should not replace medication cards, approved drug references, instructor guidance, or facility policy.
| Cardiac medication class | Think about | Nursing student reminder |
|---|---|---|
| Beta blockers | Rate, pressure, workload | Check pulse/BP as required and assess symptoms. |
| ACE inhibitors/ARBs | Pressure, renal function, potassium | Watch BP trends, potassium, renal context, dizziness. |
| ARNIs | Heart failure context, pressure, renal/electrolytes | Follow current references and policy. |
| Calcium channel blockers | Pressure, vascular tone, sometimes rate | Do not assume every drug in the class acts the same. |
| Diuretics | Fluid, weight, electrolytes | Track I&O, daily weight where ordered, edema, labs. |
| Nitrates/vasodilators | Workload, vessels, symptoms | Watch BP, dizziness, headache, response. |
| Anticoagulants/antiplatelets | Clot prevention, bleeding risk | Assess bruising, bleeding, stool/urine changes, falls. |
| Antiarrhythmics | Rhythm context | Monitor pulse, BP, ECG context where assigned. |
| Digoxin | Pulse, potassium, renal function, toxicity awareness | Do not use universal hold rules; follow order and policy. |
| Statins | Lipids, adherence, muscle symptoms | Teach reporting of muscle symptoms as directed. |
| SGLT2 inhibitors | Cardiac/renal/endocrine overlap | Monitor volume, renal function, glucose context where relevant. |
| MRAs | Potassium, renal function, fluid status | Recognize hyperkalemia and renal context as safety concerns. |
Monitoring Patients Receiving Cardiac Medications
Monitoring cardiac medications requires connecting the ordered medication with the patient’s assessment findings. A good nursing student does not simply ask, “Was the medication given?” A stronger student asks, “What assessment findings matter before and after this medication?”
| Monitoring area | What nurses may assess | Why it matters |
|---|---|---|
| Blood pressure | Baseline, current value, trend, symptoms | Many cardiac medications lower BP or affect workload. |
| Pulse | Rate, rhythm regularity, symptoms | Some medications affect heart rate or conduction. |
| Apical pulse | When required by order, policy, or medication | May be important for rate-affecting drugs. |
| ECG/rhythm context | Rhythm strip, telemetry status, ordered monitoring | Helps connect medication effect with rhythm safety. |
| Oxygen saturation | Current value and trend | Cardiac and respiratory symptoms can overlap. |
| Respiratory status | Shortness of breath, work of breathing, lung sounds | Fluid overload or poor cardiac response may appear clinically. |
| Edema | Location, severity, trend | Helps evaluate fluid status. |
| Lung sounds | Crackles or changes where relevant | May relate to fluid balance and cardiac status. |
| Daily weight | Weight trend where ordered | Useful for fluid-status monitoring. |
| Intake/output | Urine output and fluid balance | Important with diuretics and renal context. |
| Renal function | Ordered creatinine/eGFR/BUN where assigned | Affects medication safety and clearance. |
| Electrolytes | Potassium, sodium, magnesium, calcium | Electrolyte shifts can affect rhythm and drug safety. |
| Bleeding signs | Bruising, bleeding gums, stool/urine changes | Important with anticoagulants and antiplatelets. |
| Dizziness/falls risk | Orthostatic symptoms, gait, weakness | Hypotension can increase fall risk. |
| Chest discomfort reports | Location, timing, associated symptoms | Report according to policy and patient condition. |
| Medication response | Symptom improvement or worsening | Helps evaluate therapeutic response. |
| Adverse effects | New or worsening symptoms | Supports early reporting and safety. |
| Patient understanding | Ability to explain medication purpose and precautions | Helps identify education needs. |
Cardiac Medications and Vital Signs
Many cardiac medications affect blood pressure, pulse, respirations, oxygen saturation, or symptoms. Vital signs are not just numbers to record. They are clinical cues.
A blood pressure reading should be interpreted with baseline trends, posture, symptoms, medication timing, fluid status, and patient condition. A pulse reading should be interpreted with rhythm, symptoms, medication class, and ordered monitoring requirements.
For example, a patient with dizziness and a low blood pressure trend after an ordered vasodilator requires a different level of concern than a patient with a stable baseline and no symptoms. A patient with fatigue and a lower-than-usual pulse before a rate-affecting medication may require clarification before administration.
Students can review vital signs when studying cardiac medication monitoring because blood pressure, pulse, respirations, oxygen saturation, and symptom trends are central to safe nursing practice.
Do not use universal hold parameters. Follow the medication order, facility policy, approved drug reference, instructor guidance, and clinical supervision.
Cardiac Medications and Laboratory Monitoring
Laboratory monitoring depends on the medication, order, diagnosis, facility policy, and patient condition. Labs may include renal function, electrolytes, liver enzymes, coagulation tests, drug levels, lipid panels, or glucose-related values.
| Lab category | Why it may matter | Medication examples connected to the concept |
|---|---|---|
| Renal function | Some drugs affect or depend on kidney function | ACE inhibitors, ARBs, ARNIs, diuretics, digoxin, MRAs, SGLT2 inhibitors |
| Potassium | High or low potassium can affect rhythm and medication safety | Diuretics, ACE inhibitors, ARBs, ARNIs, MRAs, digoxin context |
| Sodium | Fluid and electrolyte balance may affect symptoms | Diuretics and selected cardiac contexts |
| Magnesium/calcium | Electrolyte status may affect rhythm context | Antiarrhythmics and rhythm-related concerns where ordered |
| Coagulation tests | Some anticoagulants require ordered lab monitoring | Warfarin and selected anticoagulation contexts |
| Drug levels | Some medications may require ordered serum levels | Digoxin where ordered |
| Liver-related labs | Some medications may require monitoring where ordered | Statins and other medications depending on reference guidance |
| Lipid panels | Used to monitor cholesterol therapy response | Statins and lipid-lowering therapy |
| Glucose-related values | Relevant when medication overlaps with endocrine care | SGLT2 inhibitors where relevant |
Nurses may review, document, or report labs according to facility policy and scope. Pharmacists and providers guide interpretation and medication adjustment. Nursing students should not independently adjust cardiac medications based on lab values.
Cardiac Medication Side Effects and Adverse Reactions
Cardiac medication side effects vary by class. Students should not say, “All cardiac medications cause the same side effects.” A safer approach is to group adverse effects by medication class or monitoring category.
| Monitoring category | Medication classes often connected | Nursing awareness |
|---|---|---|
| Hypotension | Beta blockers, ACE inhibitors, ARBs, ARNIs, calcium channel blockers, nitrates, diuretics, vasodilators | Assess BP, dizziness, weakness, falls risk, and symptoms. |
| Bradycardia | Beta blockers, some calcium channel blockers, digoxin, some antiarrhythmics | Assess pulse, rhythm context, dizziness, fatigue, and policy requirements. |
| Dizziness/falls | BP-lowering medications, diuretics, nitrates | Assess orthostatic symptoms, mobility, and safety precautions. |
| Electrolyte changes | Diuretics, ACE inhibitors, ARBs, ARNIs, MRAs, digoxin context | Review ordered potassium, sodium, magnesium, calcium, and renal context. |
| Renal function changes | ACE inhibitors, ARBs, ARNIs, diuretics, MRAs, digoxin, SGLT2 inhibitors | Review ordered labs and report concerns according to policy. |
| Bleeding risk | Anticoagulants, antiplatelets | Assess bruising, bleeding, stool/urine changes, and fall risk. |
| Edema | Some calcium channel blockers and cardiac conditions | Assess location, severity, trend, and related symptoms. |
| Cough/angioedema awareness | ACE inhibitors | Recognize cough as a possible issue and angioedema as a safety concern. |
| Muscle symptoms | Statins | Teach patients to report new or severe muscle symptoms as directed. |
| Digoxin toxicity awareness | Digoxin | Watch for concerning symptoms, renal/electrolyte context, pulse concerns, and ordered levels. |
| Administration reactions | IV or high-alert contexts where applicable | Follow route, rate, compatibility, and policy guidance. |
Students should use approved drug references for medication-specific details. The purpose of this article is to support nursing pharmacology learning, not patient-specific treatment decisions.
Patient Education for Cardiac Medications
Patient education for cardiac medications should be clear, practical, and within nursing scope. Students should reinforce provider instructions, pharmacist counseling, medication labels, and facility-approved education materials.
General patient education may include:
- Take medications exactly as prescribed.
- Do not stop cardiac medications suddenly unless instructed by the provider.
- Keep an updated medication list.
- Ask a provider or pharmacist before taking new OTC medications, supplements, or herbal products where relevant.
- Report dizziness, fainting, swelling, bleeding, shortness of breath, chest discomfort, severe weakness, palpitations, or other concerning symptoms according to instructions.
- Follow ordered lab appointments, blood pressure checks, weight monitoring, diet guidance, fluid guidance, or activity guidance where applicable.
- Avoid sharing medications.
- Understand when and how to seek help for concerning symptoms.
Patient Education by Medication Category
| Medication category | Patient education focus |
|---|---|
| Blood pressure medications | Take as prescribed, report dizziness or fainting, follow BP monitoring instructions where ordered. |
| Rate-affecting medications | Report unusual fatigue, dizziness, fainting, palpitations, or symptoms as instructed. |
| Diuretics | Follow weight, fluid, diet, and lab instructions where ordered; report severe weakness, dizziness, or swelling changes. |
| Anticoagulants/antiplatelets | Report bleeding concerns, bruising, blood in stool/urine, or prolonged bleeding; avoid new OTC products unless approved. |
| Statins | Report new or severe muscle symptoms as instructed; keep follow-up labs where ordered. |
| Digoxin | Follow pulse, lab, and symptom-reporting instructions where ordered; report concerning symptoms promptly. |
| SGLT2 inhibitors | Follow hydration, renal, glucose, and symptom guidance from provider/pharmacist where relevant. |
Students should avoid giving independent drug-specific instructions unless those instructions come from provider orders, pharmacist counseling, medication labels, facility policy, or approved patient education materials.
What Nurses Do Not Decide Independently With Cardiac Medications
Nurses have a major role in medication safety, but they do not independently prescribe or manage cardiac medication therapy outside orders, authorized protocols, facility policy, and scope.
They do not independently:
- Diagnose cardiac conditions.
- Choose cardiac medications.
- Set medication doses.
- Determine medication combinations.
- Start cardiac medications.
- Stop cardiac medications.
- Hold cardiac medications without order or policy support.
- Restart cardiac medications.
- Switch one medication for another.
- Titrate or adjust cardiac medications.
- Manage anticoagulation protocols independently outside policy and orders.
- Provide independent heart failure, hypertension, or arrhythmia medication plans.
- Give patient-specific treatment advice.
Nurses support safe therapy through assessment, order verification, administration, monitoring, communication, patient education, and documentation.
Cardiac Medication Documentation in Nursing
Cardiac medication documentation should show what was given, what was assessed, how the patient responded, what education was provided, and who was notified when needed.
Document according to facility policy:
- Medication administration on the MAR.
- Blood pressure and pulse checks when relevant.
- Apical pulse if required.
- Relevant labs reviewed within nursing role.
- Patient response.
- Adverse reactions or concerning symptoms.
- Patient education.
- Provider, pharmacist, RN, instructor, or preceptor notification where required.
- Held, delayed, clarified, refused, or omitted medications according to policy and order context.
Avoid vague documentation such as “patient fine” or “medication given.” Use objective language and facility-approved abbreviations.
Documentation Examples
| Situation | Stronger documentation example |
|---|---|
| Routine administration | “Medication administered per MAR after BP and pulse reviewed according to policy.” |
| Apical pulse required | “Apical pulse assessed before ordered cardiac medication; finding documented per facility process.” |
| Dizziness after medication | “Patient reported dizziness after ordered medication; BP assessed, safety maintained, RN/provider notified per policy.” |
| Bleeding concern | “Patient reported prolonged bleeding from small cut while taking ordered anticoagulant; RN/provider notified and education reinforced.” |
| Medication refusal | “Patient refused ordered cardiac medication, stating concern about dizziness; RN notified, education provided within scope, refusal documented.” |
| Clarified order | “Medication order clarified with RN/preceptor before administration due to unclear parameter.” |
| Patient education | “Education provided on reporting dizziness, bleeding, swelling, shortness of breath, or chest discomfort according to discharge instructions.” |
| Lab concern | “Ordered lab result reviewed within role; concern reported to RN/instructor per facility process.” |
Good documentation supports patient safety, communication, legal accountability, and continuity of care.
Common Cardiac Medication Mistakes Nursing Students Make
| Mistake | Why it matters | Safer habit |
|---|---|---|
| Memorizing drug names without class understanding | Names alone do not guide monitoring | Learn class, expected effect, and safety checks. |
| Ignoring pulse or blood pressure checks | Rate and BP changes may affect safety | Review required assessments before administration. |
| Using universal hold parameters | Policies and orders differ | Follow provider order, facility policy, and instructor guidance. |
| Missing electrolyte context | Electrolytes affect rhythm and medication safety | Review potassium, sodium, magnesium, and calcium where ordered. |
| Forgetting renal function relevance | Renal changes may affect medication clearance or safety | Connect renal labs to medication context. |
| Missing bleeding risk | Anticoagulants and antiplatelets require bleeding awareness | Assess bruising, bleeding, stool/urine changes, and falls. |
| Not recognizing orthostatic/fall risk | Hypotension can lead to injury | Ask about dizziness and use safety precautions. |
| Confusing side effect and allergy without clarification | Incorrect documentation can affect future care | Clarify reaction details according to policy. |
| Assuming all drugs in a class have identical effects | Some classes include different medication effects | Use approved medication references. |
| Not connecting symptoms to medication effects | New symptoms may signal adverse effects | Reassess, document, and report concerns. |
| Thinking nurses choose or adjust cardiac medications independently | This violates scope and safety principles | Stay within orders, policy, and scope. |
| Documenting without assessment context | Poor documentation weakens continuity of care | Include relevant vitals, symptoms, education, and notifications. |
Cardiac Medications and Nursing Clinical Judgment: Cue Clustering Examples
Clinical judgment means looking at cues together rather than reacting to one detail. A medication name, vital sign, symptom, and lab value may mean more when viewed as a pattern.
Example 1: Low Pulse Before an Ordered Rate-Affecting Medication
Scenario: A patient has an ordered rate-affecting cardiac medication.
Objective cues: Pulse is lower than the patient’s usual trend. Blood pressure is also lower than earlier readings.
Subjective cues: The patient reports unusual fatigue.
Cardiac medication context: Some cardiac medications can lower heart rate and blood pressure.
Possible nursing concern: The concern is not the pulse alone. The concern is the cluster of a rate-affecting medication, lower-than-usual pulse, lower blood pressure trend, and fatigue.
Appropriate student action: Reassess according to instruction, do not guess, notify the RN/instructor/preceptor, follow facility policy, and document findings and communication.
Example 2: Dizziness and Low Blood Pressure After Medication
Scenario: A patient received an ordered blood pressure medication earlier.
Objective cues: Blood pressure is lower than baseline. The patient appears unsteady when standing.
Subjective cues: The patient reports dizziness.
Cardiac medication context: Some cardiac medications may contribute to hypotension or orthostatic symptoms.
Possible nursing concern: Fall risk and symptomatic hypotension.
Appropriate student action: Maintain safety, assist within role, report to the nurse or instructor, reassess as directed, and document symptoms and communication.
Example 3: Bleeding Concern in a Patient Taking an Ordered Anticoagulant
Scenario: A patient is taking an ordered anticoagulant.
Objective cues: New bruising appears on the arms. The patient’s urine appears darker than usual.
Subjective cues: The patient says bleeding from a small cut took longer than expected.
Cardiac medication context: Anticoagulants increase bleeding-risk concerns.
Possible nursing concern: Possible bleeding complication.
Appropriate student action: Report promptly according to policy, avoid giving independent medication instructions, document assessment findings, and reinforce provider/pharmacist instructions.
Example 4: Electrolyte Concern in a Patient Receiving a Diuretic
Scenario: A patient is receiving an ordered diuretic.
Objective cues: Recent ordered labs show an electrolyte value outside the expected range. Intake/output has changed.
Subjective cues: The patient reports weakness.
Cardiac medication context: Diuretics can affect fluid balance and electrolytes.
Possible nursing concern: Electrolyte-related safety issue.
Appropriate student action: Notify the RN/instructor/preceptor, follow policy for reporting labs, document findings, and do not independently adjust medication or electrolytes.
Example 5: Digoxin Toxicity Concern at a Nursing-Student Level
Scenario: A patient is taking ordered digoxin.
Objective cues: Renal function and potassium are being monitored. Pulse assessment is required by policy.
Subjective cues: The patient reports nausea and unusual weakness.
Cardiac medication context: Digoxin safety requires attention to pulse, renal function, potassium, symptoms, and ordered levels.
Possible nursing concern: Potential digoxin-related adverse effect or toxicity concern.
Appropriate student action: Reassess, notify the RN/instructor/provider according to policy, document symptoms and findings, and avoid giving dosing or treatment advice.
When to Report Concerns During Cardiac Medication Therapy
Report concerns according to facility policy, instructor or preceptor guidance, provider orders, pharmacist guidance, and patient condition.
Students should report:
- Abnormal vital signs according to policy.
- Symptomatic hypotension.
- Low pulse concerns according to order or policy.
- New rhythm changes if assigned to monitor.
- Bleeding concerns.
- Severe dizziness or fall risk.
- Electrolyte concerns where assigned to review labs.
- Renal function concerns where assigned to review labs.
- New or worsening adverse effects.
- Patient refusal.
- Missed doses.
- Unclear medication orders.
- Possible medication allergy or reaction.
- Patient misunderstanding of medication instructions.
Escalate uncertainty rather than guessing. Document communication according to facility policy.
How to Study Cardiac Medications for Nursing School
The best way to study cardiac medications is to learn by class first. Long drug lists can overwhelm students, but medication classes create structure.
Use this study framework:
| Study step | What to ask yourself |
|---|---|
| Identify the class | Is this a beta blocker, diuretic, anticoagulant, statin, ACE inhibitor, or another class? |
| Know the general purpose | What cardiovascular problem may this medication support when ordered? |
| Connect to vital signs | Does it affect BP, pulse, rhythm, oxygenation, or symptoms? |
| Connect to labs | Does it require renal, electrolyte, coagulation, liver, lipid, glucose, or drug-level awareness? |
| Identify adverse effects | What class-related problems should a nurse monitor? |
| Plan patient education | What should the patient know within nursing scope? |
| Practice documentation | What assessment and response details should be documented? |
| Use case studies | Can you connect the medication to patient cues? |
| Ask for guidance | What does your instructor, facility policy, or drug reference emphasize? |
Students can also compare pharmacokinetics vs pharmacodynamics to understand the difference between how the body handles a drug and how the drug affects the body.
When to Ask for Help With Cardiac Medication Assignments
Cardiac medication assignments can be difficult because they combine pharmacology, health assessment, pathophysiology, medication administration, patient education, and documentation. Students may need help with medication cards, nursing pharmacology assignments, case studies, care plans, patient education plans, clinical reflections, or medication-safety questions.
Academic support can help students organize answers, explain nursing responsibilities, apply medication-safety concepts, and connect cardiac medications to patient cues without giving unsafe prescribing advice.
If you need structured academic help, you can review nursing assignment help or nursing case study help for support with medication cards, case studies, care plans, and clinical reasoning assignments.
FAQs About Cardiac Medications
1. What are cardiac medications?
Cardiac medications are drugs used to support heart and blood vessel conditions when ordered. They may affect blood pressure, pulse, rhythm, cardiac workload, contractility, clotting, cholesterol, fluid balance, renal function, or electrolytes. In nursing, the focus is not prescribing but safe administration, monitoring, patient education, communication, and documentation.
2. What are common cardiac medications in nursing?
Common cardiac medications nursing students may recognize include beta blockers, ACE inhibitors, ARBs, ARNIs, calcium channel blockers, diuretics, nitrates, anticoagulants, antiplatelets, antiarrhythmics, cardiac glycosides such as digoxin, statins, SGLT2 inhibitors, and mineralocorticoid receptor antagonists. Students should learn the medication class, expected effect, safety checks, adverse effects, and documentation needs.
3. What are the main classes of cardiac medications?
The main classes of cardiac medications include beta blockers, ACE inhibitors, ARBs, ARNIs, calcium channel blockers, diuretics, nitrates, anticoagulants, antiplatelets, antiarrhythmics, cardiac glycosides, statins, SGLT2 inhibitors, mineralocorticoid receptor antagonists, and selected vasodilators. Each class has different monitoring priorities, so students should avoid assuming all cardiac medications have the same effects.
4. What should nurses check before giving cardiac medications?
Nurses may check patient identity, medication order, MAR, allergies, medication label, route, time, blood pressure, pulse, rhythm context, respiratory status, renal function, electrolytes, bleeding risk, fall risk, fluid balance, patient symptoms, and facility-specific requirements. The exact checks depend on the medication, patient condition, order, policy, and scope of practice.
5. Why do nurses check pulse before some cardiac medications?
Nurses check pulse before some cardiac medications because certain drugs can affect heart rate, rhythm, or conduction. Pulse assessment may help identify concerns before administration. However, students should not apply universal hold rules. They should follow provider orders, drug references, facility policy, and instructor guidance.
6. What labs matter for cardiac medications?
Labs that may matter include renal function, potassium, sodium, magnesium, calcium, liver-related labs, coagulation tests, drug levels, lipid panels, and glucose-related values depending on the medication and order. Nurses may review and report labs according to policy, but medication adjustment belongs to provider-guided or authorized protocol-based care.
7. What are common side effects of cardiac medications?
Common side-effect categories include hypotension, bradycardia, dizziness, fall risk, electrolyte changes, renal function changes, bleeding risk, edema, cough or angioedema awareness with ACE inhibitors, muscle symptoms with statins, and toxicity awareness with digoxin. Side effects differ by medication class, so students should use approved drug references.
8. What are digoxin nursing implications?
Digoxin nursing implications include pulse assessment according to order or policy, renal function awareness, potassium context, toxicity awareness, ordered serum level awareness, patient education, and reporting concerns. Students should avoid universal pulse hold parameters, dosing advice, toxicity treatment steps, or independent serum-level interpretation.
9. Can nurses hold or adjust cardiac medications independently?
Nurses do not independently hold, stop, restart, switch, titrate, or adjust cardiac medications unless acting under provider orders, facility policy, authorized protocols, and scope of practice. Nursing students should always involve the RN, instructor, preceptor, pharmacist, or provider when unsure.
10. How should nursing students study cardiac medications?
Nursing students should study cardiac medications by class first. Connect each class to vital signs, labs, adverse effects, patient education, documentation, and clinical cues. Medication cards, case studies, approved drug references, simulation scenarios, and instructor guidance can help students move beyond memorization.
Final Thoughts on Cardiac Medications
Cardiac medications are one of the most important topics in nursing pharmacology. They require more than memorizing drug names. Nursing students must connect each medication class with blood pressure, pulse, rhythm context, renal function, electrolytes, fluid balance, bleeding risk, adverse effects, patient education, communication, and documentation.
Safe nursing practice depends on provider orders, medication labels, approved drug references, facility policy, pharmacist guidance, instructor guidance, and scope of practice. Nurses support cardiac medication therapy through assessment, order verification, safe administration, monitoring, patient teaching, timely reporting, and accurate documentation.
If students need help with cardiac medication assignments, nursing pharmacology case studies, medication cards, clinical reflection, or care plan interpretation, they can upload their instructions and rubric for academic guidance.
References
American Heart Association. (2025a, February 27). Types of heart medications. https://www.heart.org/en/health-topics/heart-attack/treatment-of-a-heart-attack/cardiac-medications
American Heart Association. (2025b, June 17). Medications used to treat heart failure. https://www.heart.org/en/health-topics/heart-failure/treatment-options-for-heart-failure/medications-used-to-treat-heart-failure
David, M. N. V., & Shetty, M. (2024). Digoxin. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK556025/
Hanson, A., & Haddad, L. M. (2023). Nursing rights of medication administration. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK560654/
Heidenreich, P. A., Bozkurt, B., Aguilar, D., Allen, L. A., Byun, J. J., Colvin, M. M., Deswal, A., Drazner, M. H., Dunlay, S. M., Evers, L. R., Fang, J. C., Fedson, S. E., Fonarow, G. C., Hayek, S. S., Hernandez, A. F., Khazanie, P., Kittleson, M. M., Lee, C. S., Link, M. S., … Yancy, C. W. (2022). 2022 AHA/ACC/HFSA guideline for the management of heart failure. Circulation, 145(18), e895–e1032. https://doi.org/10.1161/CIR.0000000000001063
Lee, P. M., & Gerriets, V. (2023). Nitrates. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK545149/
MedlinePlus. (2024, June 27). Blood thinners. U.S. National Library of Medicine. https://medlineplus.gov/bloodthinners.html
Sizar, O., Khare, S., Jamil, R. T., & Talati, R. (2024). Statin medications. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK430940/