The johns hopkins fall risk assessment tool is a critical framework for nurses, students, and researchers who struggle to accurately identify hospital patients at risk of falling, assign meaningful risk categories, and justify clinical decisions in complex inpatient environments. Without a structured and hospital-specific assessment system, fall prevention becomes inconsistent, documentation weakens, and patient safety is significantly compromised, especially among elderly patients with multiple comorbidities and fluctuating conditions.
Understanding this tool requires far more than memorizing scores. It demands a deep grasp of hospital-based application, dynamic patient risk, clinical reasoning, and how structured scoring translates into actionable interventions. This guide merges all key aspects, scoring, risk categories, real clinical use, and evidence-based evaluation, into a single, comprehensive resource designed for both academic excellence and practical application.
The Real Problem: Why Fall Risk Assessment Still Fails in Hospitals
Despite widespread use of structured tools, hospital falls remain one of the most persistent patient safety challenges globally. Inpatient falls are not minor events. They lead to fractures, extended hospital stays, increased healthcare costs, and, in severe cases, mortality. Evidence shows that falls significantly burden healthcare systems and negatively affect patient outcomes (Miake-Lye et al. 2013).
However, the root problem is not the absence of tools. It is the misapplication, misunderstanding, and inconsistent use of those tools.
In many hospital settings, clinicians either rely too heavily on intuition or use assessment tools mechanically without understanding their clinical implications. Risk scores are recorded, but interventions are not aligned. Patients are categorized, but reassessments are delayed or skipped. As a result, even high-risk patients may fall because the system fails to translate assessment into action.
The johns hopkins fall risk assessment tool was developed to address these gaps by offering a structured, hospital-based framework that connects assessment directly to intervention. If you want a broader comparison of how this tool fits within clinical practice, reviewing fall risk assessment tools used in hospitals provides additional context and helps avoid conceptual confusion when writing academically.
Why the Johns Hopkins Fall Risk Assessment Tool Matters
The johns hopkins fall risk assessment tool stands out because it is designed specifically for hospital environments where patient risk is dynamic and multifactorial. Unlike simpler screening tools, it does not rely on a narrow set of variables. Instead, it incorporates multiple domains that reflect real clinical conditions.
These domains include mobility, cognition, medication use, elimination patterns, and environmental factors such as equipment. Each of these contributes to fall risk in ways that are often interconnected. For example, a patient with impaired mobility who is also receiving sedative medication is significantly more vulnerable than a patient with only one of those risk factors.
Research supports the use of multifactorial assessment approaches, emphasizing that falls rarely result from a single cause (Ganz et al. 2013). Therefore, tools that capture multiple dimensions of risk are more aligned with real-world clinical scenarios.
Another key strength of the Johns Hopkins tool is its integration into hospital workflows. It is commonly embedded in admission assessments, nursing documentation systems, and electronic health records. This integration ensures that risk assessment becomes part of routine care rather than an isolated task.
Challenges Users Face When Applying the Tool
Despite its strengths, the johns hopkins fall risk assessment tool is frequently misunderstood. One of the most common challenges is the tendency to treat the score as a final answer rather than a starting point for clinical reasoning.
In practice, a score should trigger questions such as:
- What specific factors contributed to this score?
- How might these factors change over time?
- What interventions are required immediately?
Another major challenge is the interpretation of risk categories. Students often memorize thresholds without understanding their implications. For example, moderate risk is not a neutral category. It represents a critical stage where proactive intervention can prevent escalation to high risk.
Hospital patients further complicate the process. They often present with overlapping conditions such as polypharmacy, cognitive impairment, and post-surgical weakness. These factors interact in unpredictable ways, making fall risk highly dynamic.
From an academic perspective, many students struggle to move beyond descriptive writing. They explain how the tool works but fail to evaluate its effectiveness or apply it to real scenarios. This weakens the quality of assignments and dissertations. Structured guidance from resources such as nursing research paper help or report writing support can help bridge this gap by strengthening analytical depth.
How the Johns Hopkins Fall Risk Assessment Tool Works
The johns hopkins fall risk assessment tool uses a weighted scoring system that evaluates multiple patient-specific factors. Each factor contributes differently to the overall score, reflecting its relative importance in predicting fall risk.
Core Domains Explained
The tool assesses several key domains:
Age is included because older patients are more likely to experience reduced balance, muscle weakness, and slower reflexes. However, age alone is not sufficient to determine risk.
Fall history is one of the strongest predictors. A patient who has fallen previously is more likely to fall again, particularly if underlying causes have not been addressed.
Elimination patterns are important because frequent toileting increases unsupervised movement, especially at night when staffing may be reduced.
Medications play a major role. Sedatives, antihypertensives, and other drugs can impair balance, cause dizziness, or reduce alertness.
Patient care equipment, such as IV lines or mobility aids, can restrict movement or create physical obstacles.
Mobility is heavily weighted because it directly affects the patient’s ability to move safely.
Cognition influences awareness and decision-making. Confused patients may attempt to move without assistance.
This multifactorial structure allows the tool to reflect the complexity of hospital patients more accurately than simpler models.
Scoring System: Detailed Interpretation
The johns hopkins fall risk assessment tool assigns scores to each domain, which are then summed to produce a total score.
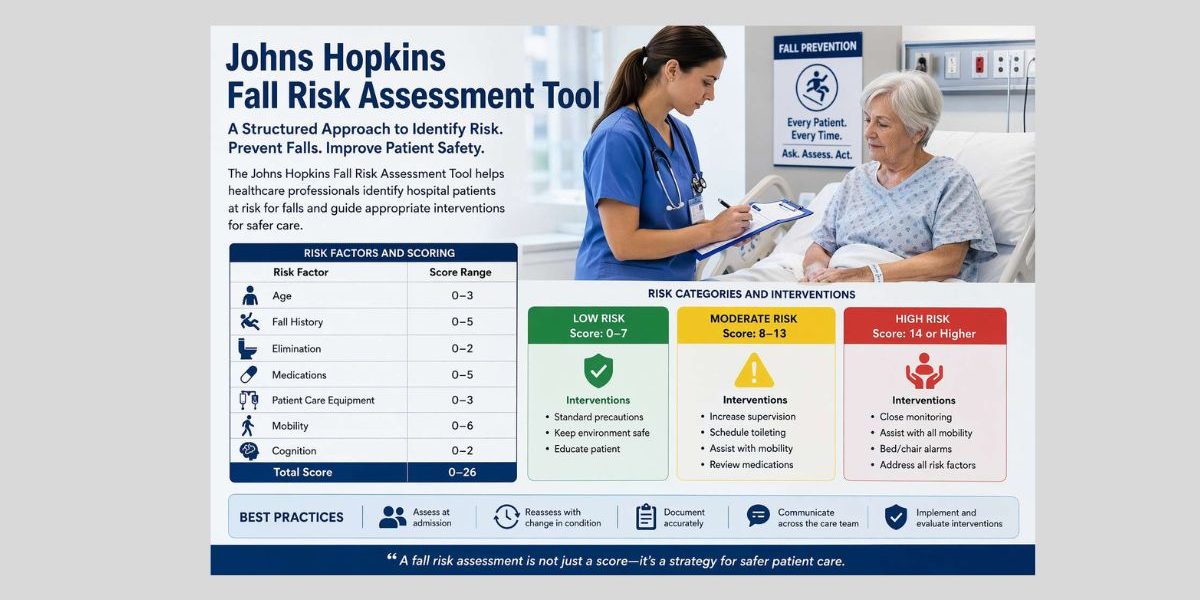
| Risk Factor | Score Range |
|---|---|
| Age | 0–3 |
| Fall History | 0–5 |
| Elimination | 0–2 |
| Medications | 0–5 |
| Equipment | 0–3 |
| Mobility | 0–6 |
| Cognition | 0–2 |
The weighted nature of the scoring system ensures that more critical risk factors, such as mobility and medication use, have a greater influence on the final score.
However, the score should never be interpreted in isolation. It must always be considered alongside clinical judgment and contextual factors.
Risk Categories and Their Clinical Meaning
The johns hopkins fall risk assessment tool categorizes patients into low, moderate, and high risk. These categories are essential because they determine intervention strategies.
Low-risk patients typically require standard precautions, such as maintaining a safe environment and providing basic education. However, this category should not lead to complacency. Even low-risk patients can fall if their condition changes.
Moderate-risk patients represent a critical intervention zone. They often retain some independence, which increases the likelihood of unsupervised movement. Therefore, proactive measures such as supervised toileting and increased monitoring are necessary.
High-risk patients require intensive intervention. This includes close supervision, assisted mobility, and environmental modifications. Research shows that linking risk categories to specific interventions improves outcomes and reduces fall rates (Miake-Lye et al. 2013).
Hospital-Based Application: A Dynamic Process
The johns hopkins fall risk assessment tool is designed for continuous use within hospital environments. It should be applied not only at admission but throughout the patient’s stay.
Risk is not static. A patient who is stable at admission may become high risk due to:
- Medication changes
- Post-surgical complications
- Cognitive decline
- Infection
For example, an elderly patient admitted for pneumonia may initially be categorized as moderate risk. After receiving sedative medication, the patient may become confused and physically weak, increasing their risk significantly. Without reassessment, this change may go unnoticed.
This dynamic nature of risk highlights the importance of regular reassessment and interdisciplinary communication.
Common Errors in Clinical Application
Even experienced clinicians make mistakes when using the johns hopkins fall risk assessment tool. One of the most common errors is treating it as a one-time assessment. This approach ignores the dynamic nature of hospital patients.
Another error is over-reliance on the score. While the tool provides valuable guidance, it cannot capture every aspect of patient risk. Environmental factors such as lighting, clutter, and staffing levels also play a role.
Poor documentation is another significant issue. Incomplete or inaccurate records can undermine both patient safety and academic credibility.
Students who struggle with applying these concepts in assignments can benefit from targeted support through case study help, which focus on translating theory into practice.
Advanced Clinical Application in Hospital Settings
The true value of the johns hopkins fall risk assessment tool becomes evident when it is applied consistently within real hospital workflows. While the scoring system provides structure, its effectiveness depends on how clinicians interpret and act on the results within dynamic care environments.
In practice, hospital settings are characterized by rapid patient turnover, fluctuating conditions, and varying levels of staffing. Under these circumstances, fall risk is not a fixed attribute but a constantly evolving state. For this reason, the Johns Hopkins framework is designed to be integrated into ongoing clinical processes rather than used as a one-time assessment.
Clinicians are expected to reassess patients at key transition points, including post-operative recovery, medication adjustments, or sudden cognitive decline. For example, a patient who was initially alert and mobile may become disoriented due to infection or medication side effects. In such cases, failure to reassess using the johns hopkins fall risk assessment tool can result in missed risk escalation and subsequent falls.
Furthermore, effective application requires interdisciplinary collaboration. Nurses, physicians, physiotherapists, and occupational therapists must interpret the tool collectively, ensuring that risk scores translate into coordinated care strategies. This collaborative approach strengthens patient safety and ensures that interventions are both timely and appropriate.
Deep Dive into Risk Categories and Intervention Mapping
While earlier sections introduced risk categories, a deeper understanding reveals how critical they are in guiding patient care. The johns hopkins fall risk assessment tool does not merely classify patients; it provides a structured pathway for intervention.
Low-risk patients, although generally stable, still require vigilance. Hospital environments are unfamiliar, and even minor changes such as dizziness from new medication can increase fall risk. Therefore, standard precautions must always be maintained.
Moderate-risk patients represent a particularly sensitive group. These individuals often retain some degree of independence, which paradoxically increases their risk. Because they feel capable of moving independently, they may attempt unsupervised activities. This highlights the importance of proactive interventions such as scheduled assistance and environmental modifications.
High-risk patients demand the most attention. These individuals typically exhibit multiple risk factors, including impaired mobility, cognitive confusion, and complex medication regimens. In such cases, interventions must be comprehensive and immediate. Continuous monitoring, assisted mobility, and environmental adjustments become essential components of care.
Research consistently demonstrates that structured intervention strategies linked to risk categories significantly reduce fall incidence (Miake-Lye et al. 2013). Therefore, the effectiveness of the johns hopkins fall risk assessment tool depends not only on accurate scoring but also on the timely implementation of appropriate interventions.
Real Clinical Case Applications
To fully understand the johns hopkins fall risk assessment tool, it is essential to examine how it operates in real clinical scenarios.
Consider an elderly patient recovering from surgery. Initially, the patient may be alert but physically weak. The tool would assign points for age, mobility impairment, and possibly medication use, placing the patient in a moderate or high-risk category. If the patient later develops confusion due to medication or infection, the risk category may escalate further, requiring immediate intervention.
In another scenario, a middle-aged patient with intravenous equipment may appear stable. However, the presence of equipment introduces environmental hazards that increase fall risk. The tool captures this nuance by assigning points for patient care equipment, ensuring that such risks are not overlooked.
Even patients categorized as low risk require careful monitoring. A seemingly stable patient may experience sudden dizziness or hypotension, particularly in the early stages of hospitalization. These examples demonstrate that the tool is not about labeling patients but about guiding continuous, context-sensitive care.
Accuracy and Evidence-Based Evaluation
The johns hopkins fall risk assessment tool is supported by evidence, yet it is important to approach its accuracy with nuance. No fall risk assessment tool can predict falls with complete certainty. Instead, these tools estimate probability based on known risk factors.
Research indicates that multifactorial tools improve the identification of at-risk patients but should not replace clinical judgment (Ganz et al. 2013). The strength of the Johns Hopkins model lies in its comprehensive approach, which captures multiple dimensions of risk.
However, its effectiveness depends on proper implementation. Inconsistent use, incomplete documentation, or lack of reassessment can significantly reduce its predictive value. Additionally, the tool may not fully account for sudden changes in patient condition, reinforcing the need for ongoing clinical evaluation.
From an academic perspective, understanding these strengths and limitations is crucial. Students must demonstrate the ability to critically evaluate the tool rather than simply describing its components. This level of analysis is often required in advanced coursework and research projects.
Common Errors in Advanced Use
Even experienced clinicians and students make errors when applying the johns hopkins fall risk assessment tool. One of the most significant mistakes is over-reliance on numerical scores. While the scoring system provides valuable guidance, it cannot capture every aspect of patient risk.
Another common error is failure to reassess. Hospital environments are dynamic, and patient conditions can change rapidly. Without regular reassessment, risk categorization becomes outdated and ineffective.
Inconsistent documentation also undermines the tool’s effectiveness. Accurate and thorough documentation ensures continuity of care and supports communication among healthcare professionals.
Students often replicate these errors in academic work by focusing on description rather than analysis. To address this, structured academic support such as coursework help for nursing students or nursing homework help can help develop deeper understanding and stronger analytical skills.
Ethical Considerations in Clinical and Academic Contexts
The ethical use of the johns hopkins fall risk assessment tool extends beyond technical accuracy. In clinical practice, healthcare professionals have a responsibility to prioritize patient safety above all else. This means using the tool as a guide rather than a substitute for clinical judgment.
Patients must be treated as individuals, not as scores. Each assessment should consider the broader context, including environmental factors and patient preferences. Over-reliance on structured tools without individualized care can lead to ethical concerns and compromised outcomes.
In academic contexts, ethical considerations include accurate representation of evidence, proper citation, and original analysis. Students must avoid misinterpreting research findings or presenting incomplete information. The emphasis should always be on critical thinking and evidence-based reasoning.
The philosophy outlined on the About Us page reflects this commitment to ethical academic support, ensuring that students receive guidance that enhances learning rather than undermines it.
Academic and Professional Support for Mastery
Mastering the johns hopkins fall risk assessment tool requires a combination of clinical understanding and academic skill. Many students find it challenging to integrate these elements, particularly when dealing with complex topics such as risk assessment and evidence evaluation.
Professional support can play a valuable role in bridging this gap. Services such as nursing assignment help provide structured guidance that helps students develop clear, well-supported arguments.
For more advanced work, including dissertations and research projects, specialized support is available through DNP dissertation help and dissertation data analysis help. These services focus on enhancing understanding and ensuring that academic work meets high standards of quality and rigor.
Transparent Process and Trust Signals
Trust is a critical factor when seeking academic support. Clear processes and transparent policies ensure that students can make informed decisions.
The process typically begins with submitting requirements through the order page. From there, experts analyze the task, develop content, and provide revisions as needed. Pricing details are available on the pricing page, and policies are outlined in the refund policy.
These elements contribute to a reliable and professional service experience.
Frequently Asked Questions
A common question is whether the johns hopkins fall risk assessment tool can prevent all falls. The answer is no. While it significantly reduces risk, it cannot eliminate it entirely. Falls are influenced by numerous factors, some of which may not be captured within the tool.
Another frequent question concerns accuracy. The tool is effective in identifying at-risk patients, but it must be used alongside clinical judgment. It is not a predictive guarantee but a structured guide.
Users also ask how often the tool should be applied. The answer depends on patient condition. In general, it should be used at admission and reassessed whenever there is a significant change.
Finally, many students ask whether the tool is better than others. The answer is context-dependent. While the Johns Hopkins model is comprehensive, its effectiveness depends on proper implementation and the specific clinical environment.
Final Call to Action
If you are struggling to fully understand or apply the johns hopkins fall risk assessment tool, you are not alone. Many students and professionals find it difficult to connect scoring systems, clinical application, and academic analysis. What you need is structured, expert guidance that transforms complexity into clarity. Whether you are working on assignments, case studies, research papers, or dissertations, the right support can help you produce high-quality, evidence-based work that stands out. You can explore real examples on the samples page or begin your project through the order page.
Final Conclusion
The johns hopkins fall risk assessment tool is more than a scoring system. It is a comprehensive clinical framework that supports patient safety, enhances decision-making, and strengthens academic understanding.
Its effectiveness depends on how well it is applied. When used correctly, it enables healthcare professionals to identify risk, implement targeted interventions, and improve patient outcomes. When misunderstood, it becomes just another checklist.
Mastering this tool means mastering a critical aspect of hospital patient safety and positioning yourself for both clinical and academic success.
References
Ganz, David A., Xinhui Huang, Steven L. Saliba, and John T. Shier. 2013.
“Preventing Falls in Hospitals: A Toolkit for Improving Quality of Care.”
Agency for Healthcare Research and Quality (AHRQ).
https://pubmed.ncbi.nlm.nih.gov/23624504/
Miake-Lye, Ira M., Paul A. Hempel, Beverly Ganz, and Sidney Dy. 2013.
“Inpatient Fall Prevention Programs as a Patient Safety Strategy: A Systematic Review.”
Annals of Internal Medicine 158 (5 Pt 2): 390–396.
https://pubmed.ncbi.nlm.nih.gov/23460060/