Pharmacokinetics vs pharmacodynamics is one of the most important comparisons nursing students learn in pharmacology. Many students memorize the shortcut: pharmacokinetics is “what the body does to the drug,” while pharmacodynamics is “what the drug does to the body.” That definition is useful, but it is not enough.
In nursing school, you need to apply the difference to medication timing, onset, peak effect, duration, half-life, clearance, therapeutic effect, side effects, adverse effects, toxicity, and patient monitoring. This guide explains the comparison in a practical way, with nursing examples, classification tables, case scenarios, common mistakes, and assignment-writing guidance.
Quick Answer: Pharmacokinetics vs Pharmacodynamics
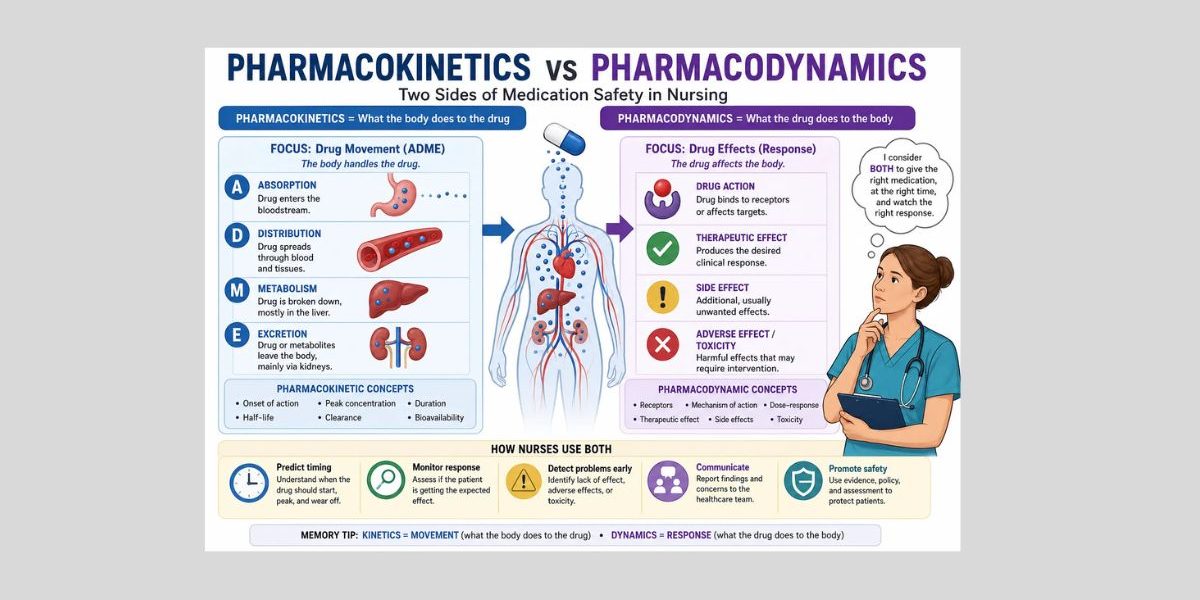
- Pharmacokinetics explains what the body does to the drug.
- Pharmacodynamics explains what the drug does to the body.
- Pharmacokinetics includes absorption, distribution, metabolism, and excretion, often called ADME.
- Pharmacodynamics includes drug action, receptors, therapeutic effects, side effects, adverse effects, toxicity, and patient response.
- Pharmacokinetics helps nurses understand timing, onset, peak, duration, half-life, clearance, and bioavailability.
- Pharmacodynamics helps nurses monitor patient response, expected effects, unexpected effects, and toxicity.
- Nursing students need both concepts to understand medication administration, monitoring, patient safety, and pharmacology assignments.
Pharmacokinetics vs Pharmacodynamics: Main Difference
The main difference is simple: pharmacokinetics follows the drug through the body, while pharmacodynamics follows the effect of the drug on the patient. Pharmacokinetics answers questions about movement and concentration. Pharmacodynamics answers questions about action and response.
| Feature | Pharmacokinetics | Pharmacodynamics | Nursing takeaway |
|---|---|---|---|
| Main question | What does the body do to the drug? | What does the drug do to the body? | Nurses need both to understand timing and response. |
| Simple meaning | Drug movement through the body | Drug effect on the body | Movement does not always equal response. |
| Major concepts | Absorption, distribution, metabolism, excretion, bioavailability, half-life, clearance | Drug action, receptors, therapeutic effect, side effects, adverse effects, toxicity | Separate ADME from patient response. |
| What nurses monitor | Timing, route, ordered labs, kidney/liver concerns, expected onset and duration | Symptom change, therapeutic response, adverse effects, toxicity signs, unexpected response | Monitoring includes both drug handling and patient condition. |
| Example | A drug is absorbed slowly after oral administration. | A patient becomes dizzy after receiving a medication. | Slow absorption is pharmacokinetic; dizziness is patient response. |
| Common student mistake | Thinking pharmacokinetics only means “absorption” | Thinking pharmacodynamics only means “side effects” | Both concepts are broader than one term. |
| Assignment use | Explain how the drug moves through the body and what affects concentration. | Explain how the drug produces effects and how the patient responds. | A strong pharmacology answer compares both, not just defines both. |
Easy Way to Remember Pharmacokinetics vs Pharmacodynamics
Pharmacokinetics means movement. Think of the word “kinetics,” which relates to motion over time. In nursing pharmacology, pharmacokinetics explains how the body handles the medication after it enters the body.
Pharmacodynamics means response. Think of “dynamics” as action, effect, or change. In nursing pharmacology, pharmacodynamics explains how the medication affects cells, tissues, organs, symptoms, and patient outcomes.
A simple memory aid is:
Kinetics = where the drug goes.
Dynamics = what the drug does.
For example, if an oral medication takes time to be absorbed before entering systemic circulation, that is pharmacokinetics. If the patient later reports symptom relief, develops dizziness, or shows a stronger-than-expected response, that is pharmacodynamics.
What Is Pharmacokinetics?
Pharmacokinetics is the study of how the body absorbs, distributes, metabolizes, and excretes a drug. These four stages are often summarized as ADME. In simple nursing language, pharmacokinetics explains what the body does to the drug from the time it enters the body until it is removed.
Pharmacokinetics helps nurses understand why route, absorption, bioavailability, onset, peak, duration, half-life, clearance, liver function, kidney function, and drug interactions matter. For example, a medication may take longer to act if absorption is delayed, or drug exposure may increase if clearance is reduced.
For a deeper explanation of ADME and drug movement, read the full pharmacokinetics for nursing students guide.
In this comparison article, remember the main point: pharmacokinetics focuses on drug movement, timing, and concentration, not the patient’s clinical response itself.
What Is Pharmacodynamics?
Pharmacodynamics is the study of how a drug affects the body. In simple nursing language, pharmacodynamics explains what the drug does to the body after it reaches its site of action.
This includes drug action, receptor binding, mechanism of action, therapeutic effects, side effects, adverse effects, toxicity, and patient response. For example, if a medication lowers blood pressure, reduces pain, causes sedation, improves breathing, or produces an unexpected adverse effect, the nurse is thinking about pharmacodynamics.
For a fuller discussion of drug effects and patient response, read the complete pharmacodynamics for nursing students article.
In this comparison article, the main point is clear: pharmacodynamics focuses on the effect of the drug, not simply how the body absorbs, metabolizes, or eliminates it.
Pharmacokinetics and Pharmacodynamics Work Together
Pharmacokinetics and pharmacodynamics are different, but they work together in medication safety. A drug must usually reach the bloodstream, move to the target area, and remain available long enough to produce an effect. That movement is pharmacokinetics.
However, drug presence does not guarantee the expected response. A medication may be present in the body but produce a weak, delayed, excessive, or unexpected effect. That response is pharmacodynamics.
For example, two patients may receive the same medication category under provider orders, but they may not respond the same way. One patient may experience the expected therapeutic effect. Another may have minimal symptom improvement. Another may develop an adverse effect. The difference may relate to age, organ function, disease state, receptor sensitivity, genetics, drug interactions, or clinical condition.
That is why nursing students should not study pharmacokinetics and pharmacodynamics as isolated definitions. Nurses monitor when the medication should begin working, when the strongest effect might occur, how long the effect may last, and how the patient actually responds.
ADME vs Drug Response
ADME belongs to pharmacokinetics. Drug response belongs to pharmacodynamics. This distinction helps students avoid one of the most common mistakes in nursing pharmacology: mixing up drug movement with drug effect.
Absorption can affect when a response begins. Distribution can affect where the drug travels. Metabolism and excretion can affect how long drug exposure lasts. However, the actual clinical response, such as pain relief, blood pressure change, sedation, nausea, rash, or toxicity, belongs to pharmacodynamics.
| Concept | Pharmacokinetic side | Pharmacodynamic side | Nursing example |
|---|---|---|---|
| Absorption | Drug moves from administration site into circulation. | Patient may begin to show a response after enough drug reaches the action site. | A delayed oral absorption pattern may delay symptom improvement. |
| Distribution | Drug moves through blood and tissues. | Effects occur when the drug reaches relevant target sites. | A drug may circulate, but the nurse still monitors whether the expected effect appears. |
| Metabolism | The body breaks down the drug, often through liver processes. | The patient may have stronger or weaker effects depending on active drug exposure. | Reduced metabolism may increase risk for adverse effects in some situations. |
| Excretion | The body removes drug or metabolites, often through the kidneys. | Drug effects may last longer if exposure increases. | A patient with reduced renal function may need closer monitoring according to orders and policy. |
| Receptors | Not an ADME process. | Drug binds to or affects targets that produce response. | A medication may lower blood pressure because of its action on cardiovascular targets. |
| Patient response | Not the movement of the drug. | The clinical effect seen in the patient. | The nurse reassesses symptoms, vital signs, adverse effects, and safety concerns. |
Onset, Peak, Duration, and Patient Response
Onset, peak, and duration are commonly discussed with pharmacokinetics because they relate to timing. They help nurses understand when a medication may start working, when the strongest concentration or effect may occur, and how long the medication may continue to produce an effect.
However, patient response is pharmacodynamic. If a patient reports pain relief, becomes overly sedated, develops dizziness, or shows no expected improvement, the nurse is looking at the drug’s effect on the body.
A key nursing point is that peak concentration is not always the same as peak clinical effect. A drug may reach a high concentration in the bloodstream, but the patient’s visible response may depend on receptor activity, disease state, tolerance, organ function, interactions, and the patient’s condition.
This is why reassessment matters. Nurses do not only ask, “When should this medication work?” They also ask, “What response am I seeing in this patient, and is that response expected, absent, excessive, or concerning?”
Half-Life, Clearance, and Toxicity Risk
Both half-life and clearance are pharmacokinetic concepts. Half-life describes how long it takes for the amount of drug in the body or plasma concentration to decrease by a certain proportion. Clearance describes how the body removes a drug from circulation.
Toxicity is a pharmacodynamic outcome because it describes a harmful drug effect in the patient. The connection is important: if clearance decreases, drug exposure may increase, and the risk of adverse effects or toxicity may rise.
Kidney and liver function often matter because the liver is commonly involved in metabolism and the kidneys are commonly involved in excretion. Disease states, age-related changes, dehydration, drug interactions, and clinical instability may also affect drug handling and response.
Nurses do not independently change medication doses or routes. Instead, they follow provider orders, facility policy, drug references, scope of practice, supervision requirements, and instructor guidance. They monitor ordered labs, assess patient response, watch for adverse effects, document findings, and communicate concerns to the healthcare team.
Receptors, Drug Effects, and Patient Variation
Receptor activity is pharmacodynamic because it explains how a drug produces an effect after reaching its target. A drug may bind to a receptor, block a receptor, activate a pathway, inhibit an enzyme, or produce another cellular effect. The details depend on the medication category.
Patients may respond differently because of receptor sensitivity, age, genetics, disease state, tolerance, organ function, drug interactions, or clinical condition. That is why the same medication category may produce different levels of response in different patients.
Pharmacokinetics may help explain drug levels or exposure. Pharmacodynamics helps explain what the drug does once it reaches the body’s target tissues. A nursing student needs both to understand why medication monitoring is not just about giving a drug at the correct time. It is also about assessing what happens afterward.
Is This Pharmacokinetics or Pharmacodynamics?
Use this table to practice classification. The easiest question is: “Am I describing drug movement, or am I describing drug effect?”
| Statement | Pharmacokinetics or pharmacodynamics? | Why |
|---|---|---|
| The drug is absorbed slowly after oral administration. | Pharmacokinetics | Absorption is part of ADME. |
| The patient becomes overly sedated. | Pharmacodynamics | Sedation is a patient response. |
| The liver metabolizes the drug. | Pharmacokinetics | Metabolism is part of ADME. |
| The medication lowers blood pressure. | Pharmacodynamics | Lowered blood pressure is a drug effect. |
| Kidney impairment slows drug clearance. | Pharmacokinetics | Clearance describes drug elimination from the body. |
| The drug binds to receptors. | Pharmacodynamics | Receptor activity explains drug action and response. |
| The patient develops an adverse effect. | Pharmacodynamics | An adverse effect is an unintended patient response. |
| The medication reaches peak concentration. | Pharmacokinetics | Peak concentration relates to drug level over time. |
| The patient reports no symptom improvement after the expected response window. | Pharmacodynamics | The focus is the patient’s clinical response. |
| The medication has reduced bioavailability because of first-pass metabolism. | Pharmacokinetics | Bioavailability and first-pass metabolism affect drug availability. |
Pharmacokinetics vs Pharmacodynamics Examples
These examples show how nursing students can separate drug movement from drug response in practical situations.
| Nursing situation | Pharmacokinetic issue | Pharmacodynamic issue | Nursing monitoring focus |
|---|---|---|---|
| Oral medication with delayed absorption | The medication takes longer to enter circulation. | The therapeutic response may appear later than expected. | Monitor timing, symptoms, and response according to orders and guidance. |
| IV medication with rapid systemic access | The drug enters circulation without an absorption delay. | The clinical effect may still depend on patient response and drug action. | Monitor for expected effect and unexpected adverse response. |
| Medication with narrow therapeutic window | Small changes in exposure may matter clinically. | Higher exposure may increase toxicity risk. | Monitor ordered labs, symptoms, adverse effects, and safety concerns. |
| Older adult with reduced renal function | Clearance may be reduced. | Effects or adverse effects may last longer or appear stronger. | Monitor ordered renal labs, sedation, dizziness, confusion, or other relevant responses. |
| Patient with unexpected sedation | Drug level, timing, interactions, or clearance may contribute. | Sedation is the observed drug response. | Assess level of alertness, safety risks, respiratory status if relevant, and report concerns. |
| Patient with no expected response | Absorption, timing, or distribution may affect exposure. | Lack of therapeutic effect is a response issue. | Reassess symptoms and document response without assuming the cause. |
| Interacting medications increase adverse-effect risk | Metabolism or clearance may be affected. | The patient may experience stronger effects or toxicity. | Check medication profile, follow policy, and communicate concerns. |
| Missed or extra doses affect levels and response | Drug concentration may fall or rise outside the expected pattern. | Symptoms may return, worsen, or adverse effects may appear. | Follow facility policy, document accurately, and notify the appropriate clinician or instructor. |
Case Scenario: Applying Both Concepts
Scenario
A patient receives an ordered medication for pain. The nurse needs to think about when the medication is expected to begin working, when reassessment may be appropriate according to facility policy and instructor guidance, whether the patient reports relief, and whether concerning effects such as excessive sedation or respiratory changes appear.
Pharmacokinetic considerations
The nurse considers how the medication enters the body, how quickly it may become available, when effects may be expected, and how long the medication may remain active. Route, absorption, distribution, metabolism, and excretion all relate to pharmacokinetics.
Pharmacodynamic considerations
The nurse assesses what the drug does to the patient. Pain relief is a therapeutic response. Excessive sedation, dizziness, nausea, or respiratory concerns may represent unwanted or adverse responses, depending on the medication and clinical context.
Nursing monitoring
The nurse follows provider orders, medication references, facility policy, and scope of practice. Monitoring may include pain reassessment, sedation level, respiratory status where relevant, vital signs, safety precautions, and documentation of therapeutic and adverse responses.
Student takeaway
Pharmacokinetics helps the nurse understand medication timing and drug movement. Pharmacodynamics helps the nurse understand whether the patient is improving, not improving, or developing concerning effects.
Common Mistakes Students Make
Memorizing definitions without application
Many students can repeat “what the body does to the drug” and “what the drug does to the body,” but they struggle to classify examples. A strong answer applies the definitions to timing, response, monitoring, and safety.
Confusing pharmacokinetics with pharmacodynamics
If the statement describes absorption, distribution, metabolism, excretion, half-life, clearance, or bioavailability, it is pharmacokinetics. If it describes therapeutic effect, side effect, adverse effect, toxicity, receptor action, or patient response, it is pharmacodynamics.
Treating onset and peak as pharmacodynamic effects only
Onset and peak often involve timing and concentration, so they are commonly discussed with pharmacokinetics. However, the patient’s actual clinical response is pharmacodynamic. Students should separate “when the medication is expected to act” from “what response the patient shows.”
Ignoring patient response
Medication knowledge is not complete if the nurse only knows the expected timing. The nurse must also assess whether the patient had the intended response and whether adverse effects occurred.
Assuming IV always means immediate clinical effect
IV administration gives rapid systemic access, but that does not mean every clinical effect appears instantly. The patient’s response still depends on drug action, target site, condition, and other clinical factors.
Assuming more drug always means better effect
A stronger exposure does not always mean a better response. It may increase adverse-effect or toxicity risk. Nursing students should avoid simplistic thinking and focus on safe monitoring.
Confusing therapeutic effect with therapeutic range
A therapeutic effect is the intended patient response. A therapeutic range refers to a drug concentration range used for some medications when levels are ordered and monitored. They are related but not the same.
Ignoring renal or liver function
Renal and liver function can influence drug handling. When ordered labs or clinical findings raise concern, nurses monitor carefully and communicate concerns according to policy and scope.
Ignoring receptor sensitivity and patient variation
Two patients may not respond the same way. Receptor sensitivity, tolerance, age, genetics, disease state, interactions, and organ function may affect response.
Writing the wrong type of answer
If the question asks about pharmacokinetics, do not write only about therapeutic effects. If the question asks about pharmacodynamics, do not write only about ADME. Use the question wording to guide your answer.
How Nurses Use Pharmacokinetics and Pharmacodynamics Together
Nurses use both concepts during medication administration, reassessment, documentation, and communication. The nurse’s role depends on scope of practice, clinical setting, provider orders, facility policy, drug references, and instructor expectations.
Nurses use pharmacokinetics when they:
- Verify medication timing and route.
- Consider expected onset, peak, and duration.
- Recognize that absorption may vary by route and patient factors.
- Understand that metabolism and excretion affect drug exposure.
- Monitor ordered labs when relevant.
- Consider kidney and liver function.
- Notice possible interaction concerns.
- Document medication timing accurately.
Nurses use pharmacodynamics when they:
- Monitor therapeutic effect.
- Watch for side effects and adverse effects.
- Assess toxicity concerns.
- Reassess symptoms after medication administration.
- Evaluate unexpected or absent response.
- Communicate patient response to the healthcare team.
- Educate patients within nursing scope.
- Document the patient’s actual response.
Together, these concepts support medication safety. Pharmacokinetics helps nurses anticipate when and how drug exposure may occur. Pharmacodynamics helps nurses evaluate what that exposure does to the patient.
Pharmacokinetics vs Pharmacodynamics in Nursing Assignments
In assignments, the best approach is to compare the two concepts instead of defining them separately and stopping there. Show how drug movement connects to drug response.
| Assignment type | How to discuss the comparison | Example focus |
|---|---|---|
| Pharmacology assignment | Define both concepts, then compare ADME with drug response. | Explain why absorption affects timing while receptors affect response. |
| Medication case study | Identify the pharmacokinetic issue and the pharmacodynamic outcome. | A patient has reduced clearance and develops adverse effects. |
| Nursing care plan | Connect medication monitoring to patient goals and safety. | Monitor therapeutic response and adverse effects as part of evaluation. |
| SOAP note | Include medication-related findings in objective and assessment sections when relevant. | Document symptom response, vital signs, and adverse-effect concerns. |
| Clinical reflection | Reflect on how medication timing and patient response shaped nursing judgment. | Discuss why reassessment mattered after administration. |
| Patient education assignment | Explain expected effects and safety monitoring in patient-friendly language. | Teach the patient what to report, within scope and policy. |
| Research paper | Use sources to explain PK/PD concepts and nursing implications. | Compare medication exposure, therapeutic response, and safety monitoring. |
| Discussion post | Answer the prompt directly, then add a nursing example. | Classify onset as timing and therapeutic effect as response. |
For students who need structured academic support, pages such as nursing assignment help or nursing case study help can fit naturally when discussing pharmacology assignments, case studies, SOAP notes, or care plan writing.
Essay and Study Topics
Useful topic ideas include:
- Pharmacokinetics vs pharmacodynamics in nursing
- ADME vs drug response
- Onset and patient response
- Half-life and toxicity risk
- Therapeutic range vs therapeutic effect
- Drug receptors and medication response
- Patient factors affecting drug effects
- Renal function and medication monitoring
- Medication route and onset of action
- Nursing responsibilities in medication monitoring
Students should narrow broad topics by medication category, patient population, pharmacology concept, safety issue, or nursing responsibility. For example, “pharmacokinetics vs pharmacodynamics” is broad. A stronger essay topic might compare drug movement and response in older adults, pain management monitoring, renal impairment, or medications with a narrow therapeutic window.
Sample Thesis Statement and Paragraph Structure
Sample thesis statement
“Pharmacokinetics and pharmacodynamics are both essential in nursing because pharmacokinetics explains how drugs move through the body, while pharmacodynamics explains how drugs affect the body and shape patient response.”
Simple paragraph structure
- Start with a topic sentence.
- Define the concept being discussed.
- Compare the pharmacokinetic and pharmacodynamic elements.
- Give a nursing example.
- Explain the monitoring or safety implication.
Sample paragraph pattern
Pharmacokinetics and pharmacodynamics help nurses understand medication safety from two different angles. Pharmacokinetics explains how the body absorbs, distributes, metabolizes, and excretes a drug, while pharmacodynamics explains the drug’s effect on the patient. For example, reduced clearance is a pharmacokinetic issue because the body removes the drug more slowly, but excessive sedation is a pharmacodynamic issue because it is a patient response. Nurses use this comparison to monitor timing, ordered labs, therapeutic effect, adverse effects, and changes in patient condition.
Quick Comparison Checklist for Nursing Students
- Am I describing what the body does to the drug? That is pharmacokinetics.
- Am I describing what the drug does to the body? That is pharmacodynamics.
- Did I mention ADME only under pharmacokinetics?
- Did I mention receptors, response, and effects under pharmacodynamics?
- Did I separate onset, peak, and duration from therapeutic response?
- Did I explain how both concepts affect monitoring?
- Did I avoid giving dosing advice?
- Did I connect the concept to patient safety?
FAQs About Pharmacokinetics vs Pharmacodynamics
1. What is the main difference between pharmacokinetics and pharmacodynamics?
Pharmacokinetics explains what the body does to the drug, including absorption, distribution, metabolism, and excretion. Pharmacodynamics explains what the drug does to the body, including therapeutic effects, side effects, adverse effects, toxicity, and patient response.
2. What is an easy way to remember pharmacokinetics vs pharmacodynamics?
Remember: kinetics means movement, and dynamics means response. Pharmacokinetics follows drug movement through the body. Pharmacodynamics follows the drug’s effect on the body.
3. Is ADME pharmacokinetics or pharmacodynamics?
ADME is pharmacokinetics. It stands for absorption, distribution, metabolism, and excretion. These stages describe how the body handles a drug.
4. Are drug receptors pharmacokinetics or pharmacodynamics?
Drug receptors are pharmacodynamics. Receptors help explain how a drug produces an effect after it reaches its target site.
5. Is onset pharmacokinetics or pharmacodynamics?
Onset is usually discussed with pharmacokinetics because it relates to timing. However, the actual clinical response that appears after onset is pharmacodynamic.
6. How do nurses use pharmacokinetics and pharmacodynamics?
Nurses use pharmacokinetics to understand timing, route, absorption, half-life, clearance, and drug exposure. They use pharmacodynamics to monitor therapeutic response, side effects, adverse effects, toxicity, and patient safety.
7. Why do nursing students confuse pharmacokinetics and pharmacodynamics?
Students often memorize definitions without practicing examples. They may also mix up timing with response. A good rule is: movement equals pharmacokinetics; effect equals pharmacodynamics.
8. How do I write about pharmacokinetics vs pharmacodynamics in an assignment?
Start by defining both terms. Then compare ADME with drug response. Add a nursing example, explain the monitoring implication, and avoid giving dosing advice or patient-specific treatment recommendations.
Final Thoughts on Pharmacokinetics vs Pharmacodynamics
Pharmacokinetics explains drug movement through the body, while pharmacodynamics explains drug effects and patient response. Nursing students need both concepts to understand medication timing, monitoring, therapeutic effect, adverse effects, toxicity, and patient safety.
The best way to master the comparison is to ask two questions. First, “Am I describing what the body does to the drug?” If yes, you are discussing pharmacokinetics. Second, “Am I describing what the drug does to the body?” If yes, you are discussing pharmacodynamics.
If students need help writing a pharmacokinetics vs pharmacodynamics essay, pharmacology assignment, medication case study, SOAP note, care plan, discussion post, or research paper, they can upload their instructions and request academic guidance.
References
Alagga, A. A., Pellegrini, M. V., & Gupta, V. (2024). Drug absorption. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557405/
Ernstmeyer, K., & Christman, E. (Eds.). (2023). Nursing pharmacology (2nd ed.). Chippewa Valley Technical College. https://www.ncbi.nlm.nih.gov/books/NBK595000/
Garza, A. Z., Park, S. B., & Kocz, R. (2023). Drug elimination. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK547662/
Grogan, S., & Preuss, C. V. (2023). Pharmacokinetics. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557744/
Marino, M., & Jamal, Z. (2023). Pharmacodynamics. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK507791/
Price, G., & Patel, D. A. (2023). Drug bioavailability. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557852/
Smith, D. A., Beaumont, K., Maurer, T. S., & Di, L. (2019). Clearance in drug design. Journal of Medicinal Chemistry, 62(5), 2245–2255. https://doi.org/10.1021/acs.jmedchem.8b01263