Surgical asepsis vs medical asepsis confuses many nursing students when they must choose the correct technique during wound care, catheterization, or OSCE stations. This article explains the difference clearly, shows when to use each approach, and helps you avoid common clinical errors that can lead to contamination, unsafe care, or lost exam marks.
Quick Answer: Surgical Asepsis vs Medical Asepsis
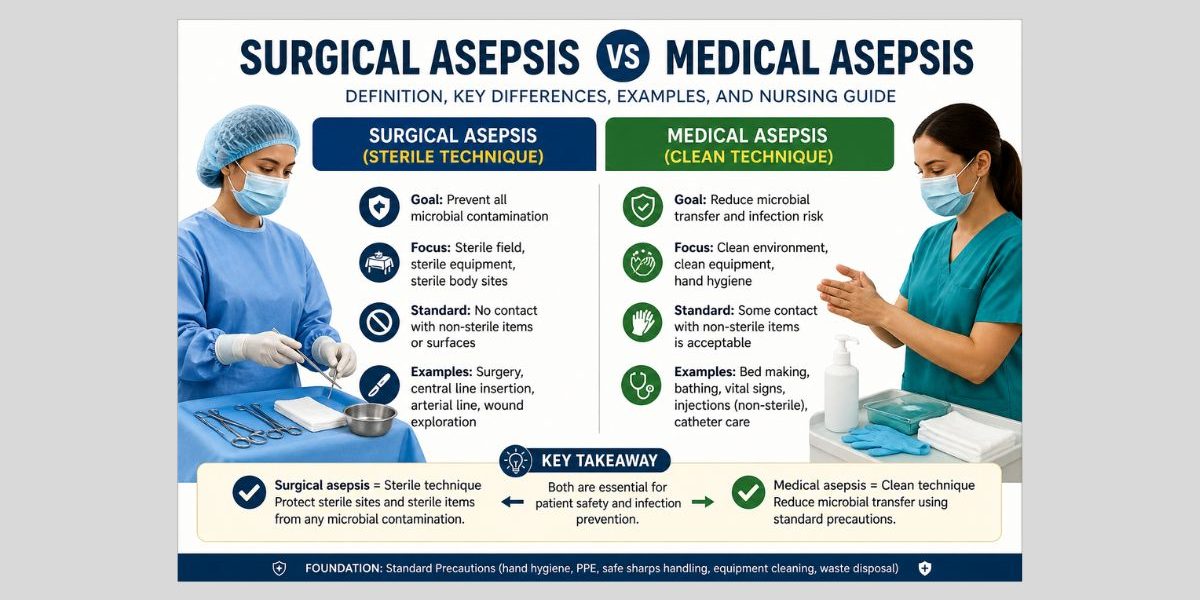
Medical asepsis means clean technique. It reduces the number and spread of microorganisms during routine care. Surgical asepsis means sterile technique. It prevents microorganisms from entering sterile body sites, wounds, sterile equipment, or invasive devices.
Use medical asepsis when caring for intact skin, cleaning equipment, handling linen, taking vital signs, or using standard precautions. Use surgical asepsis when inserting urinary catheters, changing central line dressings, preparing sterile fields, managing deep wounds, or handling sterile instruments.
| Area | Medical asepsis | Surgical asepsis |
|---|---|---|
| Main meaning | Clean technique | Sterile technique |
| Main goal | Reduce and control microorganisms | Prevent contamination of sterile areas |
| Used for | Routine care and standard precautions | Invasive or sterile procedures |
| Gloves | Usually clean gloves | Sterile gloves |
| Field required | No sterile field | Sterile field required |
| Common examples | Bed making, vital signs, equipment cleaning | Catheter insertion, sterile wound dressing, surgery |
| OSCE risk | Poor hand hygiene or glove misuse | Breaking the sterile field |
NCBI Nursing Skills describes sterile technique, or surgical asepsis, as a method clinicians use to keep objects and areas as free from microorganisms as possible during procedures that require sterility. The text lists surgical procedures, invasive wound care, and central line care as examples that require sterile technique (National Center for Biotechnology Information 2023).
Understanding the Difference Between Clean and Sterile Technique
The difference between surgical and medical asepsis is not only a textbook definition. It is a clinical decision.
Medical asepsis reduces infection risk by lowering microbial transfer. It includes hand hygiene, environmental cleaning, correct glove use, respiratory hygiene, safe sharps handling, and proper disposal of contaminated items. These practices protect patients during routine care.
Surgical asepsis goes further. It protects sterile body sites and sterile equipment from any contact with microorganisms. A non-sterile surface contaminates a sterile item on contact. The nurse must replace it.
Even small errors can harm patients, not only dramatic mistakes. Small breaks in technique can introduce organisms into a wound, catheter tract, surgical site, or vascular access point.
Healthcare workers use standard precautions for all patient care. These precautions include hand hygiene, PPE, patient-care equipment cleaning, safe injection practices, sharps disposal, and management of textiles and laundry. These actions form the base of medical asepsis (Soni 2025).
For deeper background on aseptic principles, you can also review our pillar article on the aseptic technique guide.
Why Students Struggle With Surgical Asepsis vs Medical Asepsis
Many nursing students know the definitions but struggle during clinical application. They may say surgical asepsis is sterile and medical asepsis is clean. However, they may not know what to do when a sterile catheter touches a bedsheet, when a dressing pack becomes wet, or when clean gloves touch sterile gauze. That is where clinical reasoning matters.
Students usually struggle in four areas.
First, they confuse clean with safe enough. Clean technique is appropriate for many tasks, but it is not enough for sterile body sites.
Second, they confuse gloves with sterility. Clean gloves protect against contact with body fluids, but they do not create a sterile procedure. Sterile gloves are required when the sterile field or sterile parts must be handled directly.
Third, they forget key parts and key sites. A key part is a sterile part of equipment that must not be touched. A key site is a vulnerable body site, such as a wound, insertion site, or puncture site. Aseptic non-touch technique focuses on protecting key parts and key sites from contamination during clinical procedures (Aziz 2017).
Fourth, students may panic in OSCEs. They realize they touched something non-sterile but continue the procedure. That is unsafe. In most OSCEs, it is better to identify contamination and correct it.
Medical Asepsis: Definition, Purpose, and Clinical Use
Medical asepsis is the collection of clean practices used to reduce pathogen transmission. It does not remove every microorganism. Instead, it lowers the number of organisms and prevents them from moving from one person, surface, or object to another.
Medical asepsis is used in everyday nursing care.
Examples include:
- Taking vital signs
- Assisting with bathing
- Making a patient’s bed
- Cleaning a commode
- Emptying a urinary drainage bag
- Handling used linen
- Cleaning shared equipment
- Giving oral medication
- Transporting a patient
- Removing contaminated gloves correctly
The goal is interruption of transmission. For example, when a nurse cleans a blood pressure cuff between patients, the nurse is using medical asepsis. When gloves are worn to empty a catheter bag, the nurse is using medical asepsis. When hands are cleaned before and after patient contact, that is also medical asepsis.
Hand hygiene is central because hands can transfer microorganisms between patients, surfaces, devices, and equipment. WHO hand hygiene guidance states that healthcare workers should clean hands with soap and water when visibly dirty or soiled with blood or body fluids, and hand hygiene guidance remains a major infection-prevention measure in healthcare settings.
Medical asepsis is therefore not casual hygiene. It is structured infection prevention.
Surgical Asepsis: Definition, Purpose, and Clinical Use
Surgical asepsis means sterile technique. Its purpose is to prevent microorganisms from contaminating sterile equipment, sterile fields, invasive devices, and vulnerable body sites.
It is required when microorganisms could be introduced into areas where they may cause serious harm.
Examples include:
- Urinary catheter insertion
- Central line dressing change
- Sterile wound dressing
- Surgical procedures
- Lumbar puncture assistance
- Sterile instrument preparation
- Insertion of invasive lines
- Handling sterile implants or devices
Clinicians should use sterile fields when procedures could introduce microorganisms into the patient. StatPearls identifies Foley catheter insertion, arterial line insertion, and central line placement as examples that require sterile technique (Tennant and Rivers 2022).
Surgical asepsis follows strict rules.
A sterile object remains sterile only when it touches another sterile object. The outer inch of a sterile field is usually considered contaminated unless local policy says otherwise. Sterile items below waist level or outside the nurse’s sight are no longer reliable. A wet sterile field may allow strike-through contamination. Any uncertainty should be treated as contamination.
This strictness protects patients. Surgical site infections, catheter-associated infections, and line-related infections can cause serious complications. Reviews of surgical site infection prevention emphasize strict aseptic technique as part of infection prevention (Rezaei et al. 2025).
Surgical Asepsis vs Medical Asepsis in Clinical Decision-Making
The best way to choose the correct technique is to assess the procedure risk. Do not choose based only on habit. Ask what body site, equipment, and exposure risk are involved.
Use this decision rule:
If the procedure involves intact skin and routine contact, medical asepsis is usually enough. If the procedure involves sterile sites, non-intact skin, invasive devices, sterile equipment, or key parts, surgical asepsis is usually required.
Decision-making questions
Ask these before starting:
- Will the procedure enter a sterile body cavity?
- Will it touch non-intact skin?
- Will sterile equipment enter the patient’s body?
- Are there key parts that must stay sterile?
- Is a sterile field needed?
- Could contamination cause infection or serious harm?
- Does the policy require sterile gloves or sterile instruments?
If the answer is yes to any high-risk question, prepare for surgical asepsis.
Clinical decision table
| Clinical situation | Best technique | Reason |
|---|---|---|
| Taking blood pressure | Medical asepsis | Contact with intact skin |
| Cleaning a bedside table | Medical asepsis | Environmental contamination control |
| Emptying a urinary drainage bag | Medical asepsis | Body-fluid exposure; no sterile field |
| Inserting an indwelling catheter | Surgical asepsis | Catheter enters urinary tract |
| Removing a soiled dressing | Medical asepsis | Old dressing is contaminated |
| Applying a sterile wound dressing | Surgical asepsis | Dressing contacts non-intact tissue |
| Changing a central line dressing | Surgical asepsis | Insertion site and line access must be protected |
| Helping a patient walk | Medical asepsis | Routine care |
| Preparing instruments for surgery | Surgical asepsis | Sterile field and sterile instruments required |
This table is useful for OSCEs because it turns definitions into decisions.
Key Components of Medical Asepsis
Medical asepsis has several components. Each one limits transmission.
Hand hygiene
Hand hygiene is required before and after patient contact, after body-fluid exposure risk, after removing gloves, and after touching patient surroundings. Alcohol-based hand rub is commonly used when hands are not visibly soiled. Soap and water are needed when hands are visibly dirty or contaminated with body fluids (World Health Organization 2009). In exams, students lose marks when they perform hand hygiene only at the beginning. You must repeat it at the correct moments.
Clean gloves
Clean gloves are used when exposure to blood, body fluids, mucous membranes, non-intact skin, or contaminated equipment is likely. However, gloves must be removed after the task. They should not be used to touch clean supplies, phones, keyboards, or medication carts.
Environmental cleaning
Medical asepsis includes cleaning surfaces and shared equipment. Bed rails, call bells, commodes, wheelchairs, blood pressure cuffs, and thermometers can transfer microorganisms if not cleaned properly.
Linen handling
Used linen should be handled carefully. It is crucial that you do not shake it, place it on the floor, nor hold it against your uniform. Place it directly into the correct bag or container.
Waste and sharps safety
Sharps must be disposed of immediately in approved containers. Waste should be separated according to local policy. This protects patients, staff, cleaners, and waste handlers.
Key Components of Surgical Asepsis
Surgical asepsis requires more control because sterile items must remain sterile until use.
Sterile field preparation
A sterile field must be opened on a clean, dry, stable surface. The package should be checked before opening. Do not use it if the packaging is wet, torn, expired, damaged, or uncertain.
Once the field is open, only sterile items may touch it. The nurse should avoid reaching across it, turning away from it, or allowing others to contaminate it.
Sterile gloves
Sterile gloves are required when sterile items must be handled directly. After donning sterile gloves, keep hands above waist level and in view. Do not touch masks, hair, bed rails, curtains, patient clothing, or non-sterile equipment.
If a sterile glove touches a non-sterile object, it is contaminated.
Key part and key site protection
Vital parts include catheter tips, syringe tips, sterile dressing surfaces, needle hubs, and sterile forceps tips. Key sites include wounds, insertion sites, puncture sites, and sterile body openings.
ANTT literature emphasizes key-part and key-site protection as a practical way to teach and perform aseptic procedures consistently.
Sterile transfer
Sterile supplies must be added to a field without touching the field with non-sterile packaging. Solutions should be poured without the bottle touching the sterile container. If the cap interior is touched, the solution may be unsafe.
Moisture control
A wet sterile field may become contaminated through strike-through. If fluid passes through a sterile drape or packaging, microorganisms may move from the non-sterile surface below.
What Counts as Contamination?
Students often hesitate because they are unsure whether contamination has occurred. In clinical practice, uncertainty should lead to correction.
A sterile item is contaminated when it:
- Touches a non-sterile object
- Falls below waist level
- Is outside your line of sight
- Comes from damaged packaging
- Comes from wet packaging
- Touches the outer edge of a sterile field
- Is handled with clean, not sterile, gloves
- Is exposed for too long without protection
- Is used after expiry
- Is placed on a non-sterile surface
What to say in an OSCE
If contamination happens, say:
“This item is contaminated because it touched a non-sterile surface. I will discard it and replace it before continuing.”
That statement shows safety, honesty, and clinical awareness. Trying to hide contamination is a bigger error.
Clinical Case Example 1: Urinary Catheter Insertion
A 74-year-old patient has urinary retention. The provider orders an indwelling urinary catheter. The nurse prepares a catheterization pack, performs hand hygiene, explains the procedure, positions the patient, opens the sterile field, and dons sterile gloves. This requires surgical asepsis.
The catheter enters the urinary tract. The catheter tip is a key part. The urethral opening is a key site. The sterile field, sterile gloves, lubricant, antiseptic swabs, and catheter must remain uncontaminated.
Correct clinical reasoning
The nurse must prevent microorganisms from entering the urinary tract. A contaminated catheter may increase infection risk. Therefore, sterile technique is required.
Common errors
| Error | Why it matters |
|---|---|
| Touching catheter tip with clean gloves | Contaminates a key part |
| Letting catheter touch bedding | Breaks sterility |
| Reaching over the sterile field | Risks contamination |
| Forgetting sterile glove technique | Contaminates hands before insertion |
| Continuing after contamination | Unsafe practice |
| Poor explanation to patient | Reduces consent, dignity, and cooperation |
OSCE phrase
“I am using surgical asepsis because the catheter enters a sterile body tract. I will protect the sterile field, avoid touching key parts, and replace anything that becomes contaminated.”
If you need help writing this type of clinical rationale in an assignment, our case study help can support clear, evidence-based explanations.
Clinical Case Example 2: Changing Bed Linen for a Patient With Diarrhea
A patient has diarrhea and needs a full bed change. The nurse performs hand hygiene, wears gloves and an apron, rolls soiled linen inward, avoids shaking it, places it into the correct bag, removes PPE, and performs hand hygiene again.
This requires medical asepsis.
There is no sterile field. The nurse is not inserting a device or touching a sterile body site. The goal is to prevent spread from contaminated linen to the nurse, patient, bed area, and other surfaces.
Correct clinical reasoning
The main risk is transmission through contact with contaminated linen. Clean technique, PPE, hand hygiene, and safe disposal are appropriate.
Common errors
- Shaking linen
- Carrying linen against the uniform
- Dropping linen on the floor
- Touching clean linen with contaminated gloves
- Leaving gloves on after the task
- Missing hand hygiene after glove removal
This case shows that medical asepsis is not less important. It is just different. Poor clean technique can still spread infection.
For infection-control assignments, our nursing assignment help can help you organize clinical reasoning into stronger paragraphs.
Clinical Case Example 3: Surgical Wound Dressing
A postoperative patient has an abdominal incision. The nurse removes the old dressing, assesses the wound, prepares sterile supplies, cleans the wound according to policy, and applies a new sterile dressing.
This procedure may require both medical and surgical asepsis.
Medical asepsis applies when removing the old dressing. The old dressing is contaminated. Clean gloves are used. After removal, the nurse discards the dressing, removes gloves, performs hand hygiene, and prepares for the sterile phase.
Surgical asepsis applies when opening sterile supplies and applying the new dressing. The wound is non-intact tissue. Sterile gauze, sterile forceps, sterile solution, and the wound-contact surface of the dressing must remain sterile.
Correct clinical reasoning
The old dressing is a contamination source. The new dressing must protect the wound. Therefore, the nurse changes technique during the procedure.
Common errors
| Stage | Error | Safer action |
|---|---|---|
| Removing old dressing | Using sterile gloves too early | Use clean gloves first |
| Preparing new dressing | Touching sterile gauze with clean gloves | Use sterile gloves or sterile forceps |
| Cleaning wound | Reusing contaminated swab | Use each swab once |
| Applying dressing | Touching wound-contact side | Keep contact surface sterile |
| Documentation | Writing “dressing done” only | Record wound condition and patient response |
This example is important because real nursing procedures are not always one-category tasks.
Clinical Case Example 4: Central Line Dressing Change
A patient has a central venous catheter. The transparent dressing is loose and needs replacement. The nurse gathers a sterile dressing-change kit, mask, sterile gloves, antiseptic solution, and securement supplies.
This requires surgical asepsis.
A central line provides direct vascular access. The insertion site and catheter hub are high-risk areas. Contamination can contribute to serious infection.
Correct reasoning
The procedure involves an invasive line and a key site. The dressing supplies, sterile gloves, antiseptic applicator, and catheter area must remain protected.
Common errors
- Touching the insertion site after skin antisepsis
- Allowing the catheter hub to touch bedding
- Using clean gloves during the sterile part
- Not letting antiseptic dry
- Talking directly over the exposed site without mask policy awareness
- Poor securement after dressing
Central line care is a strong example for essays because it shows why sterile technique is not optional. It directly connects aseptic practice to patient safety.
For higher-level projects, our DNP dissertation help can support infection-prevention topics, quality-improvement projects, and evidence-based practice writing.
OSCE Prep: How Examiners Mark Asepsis
OSCE examiners are not only checking whether you know the definition. They are watching your sequence, judgment, communication, correction of errors, and patient safety.
What examiners look for
| OSCE area | What earns marks |
|---|---|
| Preparation | Correct equipment and clean workspace |
| Patient safety | Identity check, consent, privacy, explanation |
| Hand hygiene | Done at correct moments |
| PPE | Appropriate for procedure risk |
| Technique choice | Clean or sterile technique justified |
| Sterile field | Opened correctly and protected |
| Key parts | Not touched or contaminated |
| Contamination response | Recognized and corrected |
| Disposal | Waste, sharps, and linen handled safely |
| Documentation | Clear, accurate, relevant |
Strong OSCE phrases
Use clear, short explanations:
- “I am using medical asepsis because this is routine care involving intact skin.”
- “I am using surgical asepsis because this procedure involves a sterile site.”
- “I will protect key parts and key sites.”
- “This sterile item is contaminated, so I will replace it.”
- “I will remove gloves and perform hand hygiene before touching clean supplies.”
- “I will maintain the sterile field above waist level and within view.”
These phrases show your reasoning without wasting time.
Common OSCE failure points
Students often fail because they:
- Touch sterile supplies with clean gloves
- Forget hand hygiene after removing gloves
- Turn away from the sterile field
- Reach over sterile items
- Continue after contamination
- Mix clean and sterile stages
- Forget to explain the procedure to the patient
- Fail to document assessment findings
The safest OSCE strategy is to slow down, verbalize risk, and correct errors immediately.
How to Write About Surgical Asepsis vs Medical Asepsis in Assignments
A strong assignment should go beyond definitions. You need to explain the clinical reason behind each technique.
Weak writing says:
Surgical asepsis prevents infection.
Better writing says:
Surgical asepsis is required during urinary catheter insertion because the catheter enters a sterile body tract. Contamination of the catheter tip may introduce microorganisms into the urinary system.
The second sentence shows decision-making. It links technique, route of contamination, and patient risk.
Use this paragraph structure
- Define the clinical procedure.
- Identify the infection risk.
- State whether medical or surgical asepsis is required.
- Explain why.
- Link to patient safety.
- Support with evidence.
For example:
A central line dressing change requires surgical asepsis because the procedure exposes a vascular access site. The catheter insertion site is a key site, and dressing materials that contact the site must remain sterile. If sterile technique is broken, microorganisms may enter the bloodstream. Therefore, the nurse must maintain a sterile field, use sterile gloves, and replace any contaminated item.
This style gives depth. It also improves marks because it shows clinical reasoning.
If you struggle to turn clinical knowledge into academic writing, our nursing research paper help can help with structure, scholarly tone, and evidence-based explanation.
Documentation After Aseptic Procedures
Documentation is part of safe care. It proves what was done, what was observed, and how the patient responded.
For a sterile wound dressing, document:
- Date and time
- Wound location
- Dressing removed
- Wound appearance
- Drainage amount
- Drainage color and odor
- Condition of wound edges
- Cleaning solution used
- Dressing applied
- Pain score
- Patient tolerance
- Education given
- Escalation if infection signs are present
For urinary catheterization, document:
- Indication
- Catheter size
- Technique used
- Urine return
- Urine appearance
- Patient tolerance
- Drainage system position
- Education given
- Any complications
Avoid vague statements such as “procedure completed.” They do not show clinical assessment.
If you need support with professional clinical writing, our clinical medical writing service and report writing services can help you improve clarity and structure.
Ethical Academic Support for Nursing Students
Academic support should help you learn, not replace your learning. That matters in nursing because assignments connect to real clinical safety.
Ethical support may include:
- Explaining complex concepts
- Reviewing outlines
- Editing grammar and flow
- Helping with literature organization
- Improving citation formatting
- Supporting data interpretation
- Building OSCE revision notes
- Giving feedback on draft structure
It should not include:
- Fabricating patient information
- Inventing clinical experiences
- Creating false references
- Encouraging plagiarism
- Writing unsafe recommendations
- Misrepresenting data
You can learn more about our academic support approach on the about us page. You can also review how it works before placing a request.
Get Help Before Your Deadline Becomes Stressful
Surgical asepsis and medical asepsis appear in nursing essays, care plans, OSCE reflections, infection-control reports, and dissertation topics. If your draft lacks depth, the issue is often not knowledge. It is structure.
You may know what clean and sterile technique mean, but still struggle to explain:
- Why one technique fits a procedure
- What contamination risk exists
- Which patient harm may occur
- How evidence supports the decision
- How to write the rationale academically
Our team can support nursing students with ethical guidance, editing, research support, and structured writing help. You can check nursing dissertation pricing or place an order when ready.
Research, Data, and Evidence-Based Projects
Some students study asepsis as part of research methods, quality improvement, or dissertation work. Topics may include hand hygiene compliance, sterile dressing audits, catheter-associated infection prevention, surgical site infection reduction, or OSCE performance after simulation training.
These projects may require quantitative or qualitative analysis.
Quantitative topics may involve:
- Infection rates before and after training
- Hand hygiene audit scores
- OSCE pass rates
- Staff compliance percentages
- Catheter-associated infection trends
For quantitative work, our SPSS data analysis help, regression analysis help, and inferential statistics help for nursing research can support data interpretation and results presentation.
Qualitative topics may involve:
- Nurses’ perceptions of aseptic technique
- Barriers to sterile field maintenance
- Student confidence during OSCEs
- Staff experiences with infection-control policies
For interview or thematic work, our qualitative data analysis support can help organize findings into clear themes. For broader dissertation support, our dissertation data analysis help can support your results chapter.
Benefits of Getting Academic Guidance on This Topic
Surgical asepsis vs medical asepsis looks simple, but high-quality writing requires clinical precision. A weak article or assignment repeats definitions. A strong one explains why the correct technique matters.
Academic guidance can help you:
- Build stronger clinical reasoning
- Use evidence accurately
- Avoid vague explanations
- Improve OSCE preparation
- Structure case examples
- Strengthen discussion sections
- Format references properly
- Improve readability
- Connect infection control to patient safety
Students who need support with shorter tasks can use nursing homework help, or coursework help for nursing students. If you need broader academic support, you can also review our affordable coursework writing service, do my nursing homework service, and samples.
Common Mistakes to Avoid in Exams and Clinical Practice
Asepsis errors often happen because students rush. The most common mistakes are predictable.
| Mistake | Why it is unsafe | Correct action |
|---|---|---|
| Using clean gloves for sterile work | Clean gloves are not sterile | Use sterile gloves when required |
| Touching sterile parts | Introduces contamination | Use non-touch technique or sterile forceps |
| Reaching over a sterile field | Contaminates sterile area | Work from the side |
| Ignoring wet packaging | Moisture may allow contamination | Replace the item |
| Keeping gloves on too long | Spreads organisms | Remove gloves after task |
| Poor hand hygiene timing | Allows transmission | Clean hands at key moments |
| Continuing after contamination | Unsafe care | Stop, discard, replace |
| Vague documentation | Weak clinical record | Record assessment and response |
These mistakes are easy to avoid once you slow down and understand the reason behind each action.
FAQs About Surgical Asepsis vs Medical Asepsis
1. What is the main difference between surgical asepsis and medical asepsis?
Medical asepsis is clean technique. It reduces the number and spread of microorganisms during routine care. Surgical asepsis is sterile technique. It prevents microorganisms from contaminating sterile fields, sterile equipment, invasive devices, and vulnerable body sites.
2. When should medical asepsis be used?
Use medical asepsis for routine patient care, environmental cleaning, non-sterile glove use, linen handling, standard precautions, and contact with intact skin. Examples include vital signs, bed making, cleaning equipment, and emptying drainage bags.
3. When should surgical asepsis be used?
Use surgical asepsis when a procedure involves sterile sites, sterile instruments, invasive devices, non-intact skin, or key parts that must remain sterile. Examples include urinary catheter insertion, sterile wound dressing, central line dressing changes, and surgery.
4. Can one procedure use both medical and surgical asepsis?
Yes. A wound dressing change often uses medical asepsis when removing the old dressing and surgical asepsis when applying the new sterile dressing. The correct technique depends on the procedure stage and contamination risk.
5. What should I do if I break sterility during an OSCE?
Stop and say what happened. For example: “This item is contaminated because it touched a non-sterile surface. I will discard it and replace it.” Recognizing contamination shows patient-safety awareness.
6. Is sterile technique always better than clean technique?
No. The best technique is the one that matches the clinical risk. Sterile technique is required for sterile sites and invasive procedures. Clean technique is appropriate for routine care and standard precautions.
Strengthen Your Nursing Assignment With Expert Support
Surgical asepsis vs medical asepsis is more than a definition. It is a clinical decision that protects patients from preventable infection. Medical asepsis controls transmission during routine care. Surgical asepsis protects sterile sites, sterile fields, and invasive devices from contamination.
For OSCEs, the key is to explain your reasoning. For assignments, the key is to connect the procedure, contamination risk, technique choice, and patient-safety outcome.
If your nursing assignment, care plan, case study, or dissertation section needs more depth, Nursing Dissertation Help can support you with ethical academic guidance. Review how it works, check pricing, or place your order for structured support.
Aziz, Abdul M. 2017. “Variations in Aseptic Technique and Implications for Infection Prevention.” British Journal of Nursing. Available through PubMed Central.
National Center for Biotechnology Information. 2023. “Chapter 4: Aseptic Technique.” Nursing Skills. NCBI Bookshelf.
Rezaei, Ahmad Reza, et al. 2025. “Surgical Site Infections: A Comprehensive Review.” Journal Article Available through PubMed Central.
Soni, S. 2025. “Infection Control.” StatPearls. NCBI Bookshelf.
Tennant, K., and C. Rivers. 2022. “Sterile Technique.” StatPearls. NCBI Bookshelf.
World Health Organization. 2009. WHO Guidelines on Hand Hygiene in Health Care. NCBI Bookshelf.