Vital signs are essential nursing assessment data, but many students struggle to move beyond memorizing “normal” numbers. In clinical practice, you must know how to measure vital signs accurately, compare them with the patient’s baseline, recognize trends, connect them with symptoms, document them correctly, and report concerning changes according to clinical guidance.
This guide covers temperature, pulse, respiratory rate, blood pressure, oxygen saturation, pain assessment where relevant, normal vital signs, pediatric and newborn considerations, orthostatic vital signs, vital signs monitors, manual versus automated readings, documentation, abnormal findings, cue clustering, and common student mistakes.
Educational safety disclaimer: This guide is for nursing education and clinical skills learning only. Vital sign assessment and response must follow facility policy, instructor guidance, provider orders, patient condition, scope of practice, and clinical judgment.
Quick Answer: What Are Vital Signs?
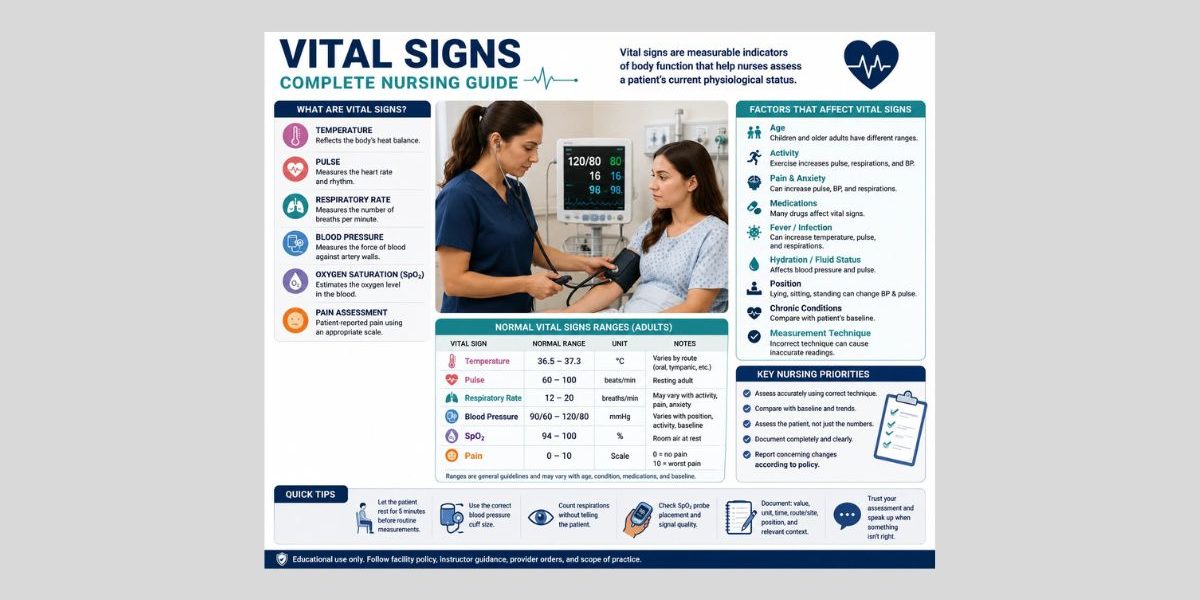
- Vital signs are measurable clinical indicators that help nurses assess a patient’s current physiological status.
- The core vital signs usually include temperature, pulse, respiratory rate, blood pressure, and oxygen saturation.
- Pain is commonly assessed alongside vital signs in many settings, depending on clinical setting and documentation requirements, but it is subjective and should not be treated as identical to objective vital signs.
- Normal vital signs vary by age, condition, activity, medication use, baseline, and measurement method.
- A single reading should be interpreted with the full patient picture, not in isolation.
- Nurses use vital signs to identify trends, recognize changes, prioritize reassessment, communicate concerns, and support patient safety.
What Are Vital Signs in Nursing?
Vital signs in nursing are measurable indicators of body function. Traditional vital signs include temperature, pulse, respiratory rate, and blood pressure. Many nursing skills references also include oxygen saturation because pulse oximetry helps nurses estimate oxygenation and interpret respiratory status more fully (Sapra et al., 2023; Ernstmeyer & Christman, 2023).
Vital signs are objective data because they are measured or observed. A pulse of 104 beats per minute, a respiratory rate of 24 breaths per minute, and a blood pressure of 96/58 mmHg are objective findings. Symptoms such as dizziness, shortness of breath, pain, weakness, nausea, or “feeling faint” are subjective data because they come from the patient’s report.
Nursing students should avoid treating vital signs as isolated numbers. A blood pressure may look acceptable on a chart but still be concerning if it has dropped sharply from the patient’s usual baseline. A respiratory rate may be “within range” but still matter if the patient is using accessory muscles, appears anxious, or reports shortness of breath.
Vital signs support nursing assessment, cue recognition, clinical judgment, reassessment, and communication. Nurses use them to answer practical questions:
- Is the patient stable compared with their baseline?
- Is the patient improving, worsening, or unchanged?
- Do the numbers match the patient’s appearance and symptoms?
- Does the reading need to be repeated manually?
- Does the nurse, instructor, preceptor, or provider need to be notified?
This is why vital signs connect closely with broader patient assessment. They are not the whole assessment, but they often provide the first measurable clues that something has changed.
Why Vital Signs Matter for Patient Safety
Vital signs matter because they can reveal early changes in patient condition. A rising respiratory rate, falling oxygen saturation, increasing pulse, new fever, or sudden blood pressure change may suggest that the patient needs reassessment. However, nursing students must interpret these findings with context, not as automatic diagnoses.
Trends often matter more than one isolated reading. For example, a pulse of 96 beats per minute may not seem alarming by itself. But if the same patient’s pulse was 72 earlier, then 84, then 96 with increasing pain and restlessness, the trend deserves attention.
Vital signs also support continuity of care. Accurate documentation helps the next nurse, instructor, provider, or clinical team member understand what was measured, when it was measured, how it was measured, and whether the patient’s condition changed.
Safety Checklist for Nursing Students
Before accepting or documenting a vital sign reading, ask:
- Does the value match the patient’s appearance?
- Was the correct technique used?
- Was the correct cuff size, route, site, or probe placement used?
- Is the patient resting, active, anxious, in pain, or recently repositioned?
- Is this value different from the patient’s baseline?
- Is the value part of a worsening trend?
- Do facility policy, provider orders, or instructor guidance require reassessment or reporting?
Measurement accuracy is important, but patient safety also depends on interpretation, communication, and follow-up.
The Main Vital Signs Nurses Assess
| Vital sign | What it measures | Common unit | Nursing focus |
|---|---|---|---|
| Temperature | Body heat balance | °C or °F | Route, fever, low temperature, infection clues, environmental effects |
| Pulse | Heart rate and pulse quality | Beats per minute | Rate, rhythm, strength, equality, baseline, symptoms |
| Respiratory rate | Breaths per minute | Breaths per minute | Rate, depth, effort, pattern, oxygen use, distress cues |
| Blood pressure | Force of blood against artery walls | mmHg | Systolic/diastolic values, cuff size, position, trends |
| Oxygen saturation | Estimated oxygen saturation of hemoglobin | SpO2 % | Signal quality, respiratory effort, oxygen device if present, symptoms |
| Pain assessment | Patient-reported pain experience | Scale or tool score | Location, quality, severity, function, reassessment requirements |
Pain needs careful wording. Pain is not always listed with the traditional vital signs, and it is not objective in the same way as temperature or blood pressure. Many clinical settings assess and document pain routinely, but pain remains subjective and should be assessed with appropriate tools and patient context. Pain can influence pulse, blood pressure, respirations, mobility, sleep, distress, and participation in care.
Normal Vital Signs Chart for Nursing Students
Normal vital signs vary by age, patient baseline, clinical condition, measurement method, route, equipment, and institutional reference ranges. The chart below is a useful student summary, not an absolute diagnostic rule. Adult ranges are commonly summarized as temperature around 36.5°C–37.3°C, pulse 60–100 beats/minute, respirations about 12–18 or 12–20 breaths/minute depending on source, and blood pressure often below 120/80 mmHg in general health references (MedlinePlus, 2025; OpenStax, 2024).
| Category | Practical student range or note | Nursing caution |
|---|---|---|
| Adult temperature | About 36.5°C–37.3°C orally in many references | Route matters; oral, tympanic, temporal, axillary, and rectal values are not interchangeable |
| Adult pulse | Common resting adult range: 60–100 bpm | Compare with baseline, rhythm, symptoms, activity, medications, pain, and anxiety |
| Adult respiratory rate | Common adult range: about 12–20 breaths/minute | Respirations are often undercounted; assess effort and pattern, not rate alone |
| Adult blood pressure | Often discussed around 90/60 to below 120/80 mmHg in general references | Interpret with baseline, posture, cuff size, symptoms, and clinical context |
| Adult oxygen saturation | Many nursing skills references use about 94%–100% as a normal learning range | SpO2 is an estimate; check signal quality and patient presentation |
| Pediatric overview | Heart and respiratory rates are usually higher in younger children than adults | Use age-specific ranges and facility pediatric references |
| Newborn overview | Newborn vital signs differ from older children and adults | Follow newborn/maternity policy and instructor guidance |
Future supporting articles such as “Normal Vital Signs” and “Vital Signs Chart” can provide more detailed normal vital signs by age, printable tables, and setting-specific study references. This pillar article gives the broader nursing assessment framework.
Vital Sign Trends vs One-Time Readings
A single vital sign can be misleading. Trends show direction.
A one-time blood pressure of 104/66 mmHg may be normal for one patient and concerning for another. A pulse of 98 may be expected after ambulation but more concerning if the patient is resting, pale, dizzy, and normally has a pulse in the 60s. A respiratory rate of 22 may be affected by pain, fever, anxiety, or respiratory illness.
When interpreting trends, compare:
- Current value with baseline
- Current value with previous readings
- Vital signs with symptoms
- Vital signs with recent activity
- Vital signs with medications
- Vital signs with pain level
- Vital signs with oxygen therapy if present
- Vital signs with patient position
- Vital signs with measurement method
A technically “normal” reading may still matter if it is far from the patient’s baseline or does not match the patient’s condition. Unexpected readings should be reassessed according to policy rather than copied without question.
Temperature as a Vital Sign
Temperature reflects the body’s heat balance. Nurses assess it to identify changes that may be associated with infection, inflammation, environmental exposure, thermoregulation problems, medication effects, or other clinical changes.
Common temperature routes include:
- Oral
- Tympanic
- Temporal
- Axillary
- Rectal, where appropriate and allowed by policy
Route matters. An axillary temperature may differ from an oral temperature. A temporal reading may be affected by technique, sweating, or device placement. A rectal temperature may be restricted in some patients or settings. Nursing students should follow facility policy and skills-lab instruction for route selection.
Factors affecting temperature include age, environment, activity, time of day, infection, inflammation, medications, recent warm or cold drinks for oral readings, and measurement route.
Documentation should include the value, unit, route, time, and relevant context. For example:
Temperature 37.8°C oral at 0800.
Do not document only “temp normal” when a precise value, route, and time are expected.
Pulse Rate as a Vital Sign
Pulse rate measures the number of palpable pulse beats per minute. Nurses also assess pulse quality when appropriate, including rhythm, strength, and equality.
Common pulse assessment sites include:
- Radial pulse
- Apical pulse
- Brachial pulse
- Pedal pulses
- Other sites based on assessment purpose and facility guidance
The radial pulse is commonly used in routine adult assessment. An apical pulse may be assessed in learning contexts, certain medication-related assessments, irregular rhythms, pediatric assessment, or when instructed by policy or preceptor guidance. For medication-related learning, vital signs may be assessed before or after medication administration depending on the medication, patient condition, and facility expectations. Students reviewing that connection can also study medication administration routes.
Factors affecting pulse include activity, fever, pain, anxiety, medications, hydration status, blood loss, cardiac conditions, body position, and oxygenation status.
Documentation may include:
Pulse 88 bpm, radial, regular.
If rhythm, strength, or site is clinically relevant or required by policy, include it.
Respiratory Rate as a Vital Sign
Respiratory rate measures breaths per minute. It is one of the most important vital signs, yet students often rush it, estimate it, or accidentally change the patient’s breathing pattern by telling the patient they are counting respirations.
A complete respiratory assessment may include:
- Rate
- Rhythm
- Depth
- Effort
- Pattern
- Breath sounds where appropriate
- Oxygen use if present
- Patient position
- Signs of distress or increased work of breathing
Respirations may be affected by activity, pain, anxiety, fever, lung disease, medications, oxygen therapy, neurological status, and metabolic changes.
Nursing students should not document a guessed respiratory rate. If the rate seems unexpected, count again according to policy and compare with patient appearance. A respiratory rate should be interpreted with oxygen saturation, work of breathing, mental status, skin color, patient report, and recent activity.
Documentation may include:
Respiratory rate 20 breaths/minute, unlabored, sitting upright.
Blood Pressure as a Vital Sign
Blood pressure measures the force of blood against artery walls. The systolic value reflects pressure during ventricular contraction, and the diastolic value reflects pressure during relaxation between beats.
Accurate blood pressure measurement depends on technique. Common causes of inaccurate readings include:
- Wrong cuff size
- Cuff placed over clothing
- Arm not supported
- Arm above or below heart level
- Patient talking during measurement
- Recent activity
- Legs crossed
- Incorrect cuff placement
- Movement during automated reading
- Repeating measurements too quickly without allowing recovery time
Cuff size matters because a cuff that is too small can produce a falsely high reading, while a cuff that is too large can produce a falsely low reading. Position also matters. Sitting, standing, lying, arm level, and recent movement can influence the value.
Manual and automated blood pressure readings both require clinical judgment. Automated readings are convenient, but unexpected readings should be checked according to policy, especially when the number does not match the patient’s appearance.
Documentation may include:
BP 118/72 mmHg, right arm, sitting, automated cuff.
Do not provide treatment conclusions from a single blood pressure reading. Interpret the value with baseline, symptoms, trend, position, medication context, and clinical guidance.
Oxygen Saturation as a Vital Sign
Oxygen saturation, commonly documented as SpO2, estimates the percentage of hemoglobin saturated with oxygen using pulse oximetry. Pulse oximetry is useful, but it has limitations.
Accuracy can be affected by poor circulation, motion, skin temperature, skin pigmentation, skin thickness, tobacco use, nail polish, artificial nails, probe placement, and poor signal quality. The FDA notes that pulse oximeter readings can be inaccurate under certain circumstances and should be interpreted with clinical context (U.S. Food and Drug Administration, 2025).
Nursing students should interpret SpO2 with:
- Respiratory rate
- Work of breathing
- Mental status
- Skin color
- Patient report of shortness of breath
- Oxygen delivery device if present
- Activity level
- Probe placement and signal quality
- Patient baseline
A low or unexpected SpO2 reading should not be ignored, but the first nursing-thinking step is to assess the patient and verify the reading according to policy. Do not give oxygen administration instructions unless you are following facility policy, provider orders, instructor guidance, and scope of practice.
Documentation may include:
SpO2 94% on room air at rest.
If the patient is receiving oxygen and policy requires it, document the delivery device and flow as applicable.
Pain Assessment and Vital Signs
Pain is often assessed alongside vital signs, but students should avoid saying pain is universally the fifth vital sign. It is subjective. The patient’s report matters, and normal vital signs do not mean pain is absent.
Pain can influence:
- Pulse
- Blood pressure
- Respiratory rate
- Sleep
- Mobility
- Appetite
- Anxiety
- Participation in care
- Recovery activities
Pain assessment tools may include numeric scales, faces scales, behavioral pain tools, age-appropriate scales, and condition-specific assessment tools. The correct tool depends on the patient, setting, developmental level, communication ability, and facility policy.
Documentation may include:
Pain 7/10, incisional, reported before ambulation.
Where required, document reassessment and communication according to policy.
Pediatric Vital Signs Overview
Pediatric vital signs vary by age. Infants beyond the newborn period, toddlers, preschoolers, school-age children, and adolescents do not share one universal “child” range.
Children often have higher heart rates and respiratory rates than adults. Younger children may also show changes in vital signs with crying, fever, anxiety, activity, pain, dehydration, or unfamiliar clinical environments. The Royal Children’s Hospital emphasizes that pediatric physiological ranges vary across publications and that patterns of change are as important as thresholds (Royal Children’s Hospital Melbourne, n.d.).
For nursing students, the key is not to force adult ranges onto children. Use age-specific references, pediatric policy, instructor guidance, and the child’s clinical presentation. A future supporting article on “Pediatric Vital Signs” can provide more detailed age-based tables and student examples.
Newborn Vital Signs Overview
Newborn vital signs differ from older children and adults. The immediate newborn and early infancy period requires attention to thermoregulation, respiratory transition, feeding behavior, color, tone, and adaptation to extrauterine life.
Newborns are especially vulnerable to heat loss because of body size, body surface area, limited reserves, and environmental exposure. Newborn respiratory patterns and heart rate should be interpreted using newborn-specific guidance, not adult or general pediatric assumptions. Open RN newborn references list newborn vital sign ranges separately, reinforcing that newborn assessment requires its own framework (Ernstmeyer & Christman, 2025).
This pillar gives only an overview. A future “Newborn Vital Signs” article can provide deeper coverage of thermoregulation, respiratory transition, newborn-specific documentation, and maternity/newborn assessment expectations.
Orthostatic Vital Signs Overview
Orthostatic vital signs are measured to assess changes related to position. Depending on policy, they may involve blood pressure and pulse measurements while lying, sitting, and standing.
They may be relevant when the patient reports dizziness, lightheadedness, weakness, falls, dehydration concerns, blood loss concerns, medication effects, or autonomic issues. The key nursing point is that orthostatic vital signs are not just numbers. They must be interpreted with symptoms, timing, position, patient safety, and facility procedure.
Students should follow facility policy for:
- Patient positioning
- Timing between position changes
- Whether lying, sitting, and standing are all required
- What symptoms to assess
- When to stop the assessment
- What to document
- When to report findings
A future “Orthostatic Vital Signs” supporting article can provide a more detailed student guide.
Manual vs Automated Vital Signs
Automated vital signs are useful in busy clinical settings, but they are not perfect. Automated devices can produce inaccurate readings when the cuff size is wrong, the patient moves, the cuff is misplaced, the rhythm is irregular, perfusion is poor, the probe signal is weak, or the equipment is not used correctly.
Manual vital signs remain important because they help students understand technique, verify unexpected readings, and build assessment confidence. Manual blood pressure, manual pulse assessment, and careful respiratory counting are still core nursing skills.
Students should not copy an unexpected automated reading without thinking. Ask:
- Does this match the patient’s condition?
- Was the equipment placed correctly?
- Was the patient moving or talking?
- Is the cuff size appropriate?
- Is the pulse oximeter waveform or signal reliable, if available?
- Should I repeat or verify manually according to policy?
Manual verification may be needed when the reading does not fit the patient’s presentation or when device accuracy is uncertain.
Vital Signs Monitor in Nursing
A vital signs monitor may measure blood pressure, pulse, oxygen saturation, and sometimes temperature. Monitors support assessment, but they do not replace nursing judgment.
Common monitor-related issues include:
- Wrong cuff size
- Motion artifact
- Poor probe placement
- Poor perfusion
- Weak pulse oximeter signal
- Device error
- Wrong patient settings
- Alarms without clinical context
- Readings that do not match the patient’s appearance
Students should assess the patient first, then interpret the monitor. A monitor can alert the nurse to possible changes, but the nurse must still evaluate the patient’s breathing, color, mental status, symptoms, pain, positioning, and overall condition.
This section is not a product review, buying guide, device comparison, or monitor recommendation. It focuses only on nursing assessment.
Factors That Affect Vital Signs
| Factor | Vital signs affected | Nursing consideration |
|---|---|---|
| Age | Temperature, pulse, respirations, BP, SpO2 | Use age-appropriate ranges, especially for pediatric and newborn patients |
| Activity | Pulse, respirations, BP, temperature | Rest before routine readings when appropriate |
| Pain | Pulse, BP, respirations | Assess pain even when objective signs look normal |
| Anxiety/stress | Pulse, respirations, BP | Consider fear, unfamiliar setting, and clinical procedures |
| Fever/infection | Temperature, pulse, respirations | Cluster with symptoms and assessment findings |
| Medications | Pulse, BP, respirations, temperature | Know medication context and facility expectations |
| Hydration/fluid status | Pulse, BP, temperature | Compare with symptoms, intake/output, and clinical picture |
| Posture | BP, pulse, SpO2 | Document position if relevant |
| Oxygen therapy | SpO2, respirations | Document oxygen device/flow if required |
| Chronic conditions | All vital signs | Compare with baseline and patient-specific history |
| Environment | Temperature, pulse, respirations | Consider heat, cold, blankets, and room conditions |
| Measurement technique | All vital signs | Incorrect technique can create false abnormalities |
| Recent procedures | Pulse, BP, respirations, pain | Interpret with timing and recovery context |
| Sleep/rest | Pulse, respirations, BP | Resting values may differ from active values |
| Caffeine/nicotine | Pulse, BP | Consider recent use where relevant |
How to Take Vital Signs Accurately
Taking vital signs accurately begins before the first measurement. Students should prepare the patient, confirm identity according to policy, explain what they are doing, use appropriate equipment, and position the patient correctly.
Practical Vital Signs Checklist
- Perform hand hygiene.
- Confirm patient identity according to facility policy.
- Explain the procedure.
- Check whether the patient has been resting, active, anxious, or in pain.
- Use the correct thermometer route and document it.
- Choose the correct blood pressure cuff size.
- Position the arm correctly for blood pressure measurement.
- Count respirations carefully.
- Check pulse rate and quality as required.
- Place the pulse oximeter correctly and assess signal quality.
- Compare readings with baseline.
- Repeat unexpected readings according to policy.
- Document value, unit, time, route/site, and relevant context.
- Report concerning findings according to policy and instructor/preceptor guidance.
This checklist does not replace skills-lab training. It helps students think through accuracy and safety.
Abnormal Vital Signs: How Nursing Students Should Think About Changes
Abnormal vital signs can mean several things. A value may be outside the expected range, changed from baseline, trending worse, inconsistent with the patient’s condition, or associated with concerning symptoms.
Do not interpret one number alone. Cluster cues.
Example 1: Elevated Pulse With Fever and Pain
A patient has a temperature of 38.4°C, pulse of 112, and reports pain of 8/10. The elevated pulse may be associated with fever, pain, anxiety, dehydration, or other clinical issues. The student should reassess, review the trend, assess symptoms, document accurately, and report according to policy.
Example 2: Low SpO2 With Increased Work of Breathing
A patient has SpO2 of 90%, respiratory rate of 26, and visible increased work of breathing. The student should not focus only on the monitor. Assess the patient, verify the reading, note respiratory effort, position, symptoms, and oxygen use if present, then report promptly according to clinical guidance.
Example 3: Blood Pressure Drop With Dizziness on Standing
A patient reports dizziness when standing, and blood pressure is lower than the previous lying or sitting value. The student should consider orthostatic context, patient safety, position, symptoms, hydration context, medications, and facility policy. Reassess and report according to guidance.
Example 4: Normal Vital Signs With Severe Pain
A patient reports pain of 9/10, but pulse and blood pressure are within expected limits. Normal vital signs do not prove pain is absent. Pain is subjective and should be assessed, documented, and communicated according to policy.
Vital Signs Documentation in Nursing
Vital signs documentation should be clear, timely, accurate, and specific. Documentation supports communication and continuity of care. Nursing documentation resources emphasize recording vital signs with relevant details such as temperature unit, route, pulse, respiratory rate, blood pressure, oxygen saturation, and pain rating when applicable (Reuter-Sandquist et al., 2022).
Document:
- Value
- Unit
- Time
- Route or site
- Patient position if relevant
- Oxygen device/flow if applicable and required
- Pain score and location if required
- Reassessment
- Communication or notification when required
- Relevant patient context
Documentation Examples
- “Temperature 37.8°C oral at 0800.”
- “BP 118/72 mmHg, right arm, sitting, automated cuff.”
- “SpO2 94% on room air at rest.”
- “Pain 7/10, incisional, reported before ambulation.”
- “Respiratory rate 22 breaths/minute, regular, sitting in chair.”
Avoid vague documentation such as:
- “Vitals okay.”
- “BP fine.”
- “Patient seems normal.”
- “O2 low.”
Use facility-approved abbreviations only.
Common Vital Signs Mistakes Nursing Students Make
| Mistake | Why it matters | Safer habit |
|---|---|---|
| Memorizing ranges without context | Normal ranges are only starting points | Compare with baseline, symptoms, and trend |
| Not comparing with baseline | A “normal” value may be abnormal for that patient | Review previous readings |
| Counting respirations inaccurately | Respiratory rate is a major safety cue | Count carefully and observe effort |
| Using the wrong cuff size | Blood pressure may be falsely high or low | Select the correct cuff |
| Documenting without route/site | The reading becomes less meaningful | Include route, site, or position when relevant |
| Ignoring pain | Pain affects function and patient experience | Assess pain with the appropriate tool |
| Assuming pain is absent because vital signs are normal | Pain is subjective | Believe and assess the patient’s report |
| Trusting monitor readings without checking patient | Devices can be wrong | Assess the patient and verify unusual readings |
| Failing to reassess abnormal readings | Errors or changes may be missed | Repeat according to policy |
| Missing trends | Worsening patterns can be subtle | Compare readings over time |
| Not reporting concerning changes | Delayed communication can affect safety | Follow parameters and instructor guidance |
| Confusing pediatric and adult ranges | Children have age-specific ranges | Use pediatric references |
| Confusing newborn and pediatric ranges | Newborn assessment is unique | Use newborn-specific guidance |
| Documenting late or vaguely | Poor documentation weakens care continuity | Chart promptly and specifically |
Vital Signs and Clinical Judgment: Cue Clustering Examples
Example 1: Fever and Tachycardia
Scenario: A postoperative patient has a temperature of 38.3°C and pulse of 110.
Objective vital sign cues: Elevated temperature, increased pulse.
Subjective patient cues: Patient reports chills and increasing incisional discomfort.
Other assessment cues: Skin warm, appears tired, pain 7/10.
Possible nursing concern: Change from baseline that may require reassessment and communication.
Appropriate student action: Recheck technique, assess pain and other symptoms, document findings, and report to the nurse, instructor, or preceptor according to policy.
Example 2: Orthostatic Dizziness
Scenario: A patient feels dizzy when standing after being in bed.
Objective vital sign cues: Blood pressure lower when standing; pulse higher than earlier reading.
Subjective patient cues: Patient reports lightheadedness.
Other assessment cues: Unsteady posture, recent reduced intake.
Possible nursing concern: Position-related vital sign change with fall risk.
Appropriate student action: Prioritize safety, follow orthostatic vital sign policy, document position and symptoms, and report according to guidance.
Example 3: Low SpO2 With Increased Work of Breathing
Scenario: A patient’s SpO2 reads 91% on the monitor.
Objective vital sign cues: SpO2 lower than prior reading, respiratory rate 26.
Subjective patient cues: Patient reports shortness of breath.
Other assessment cues: Increased work of breathing, sitting upright.
Possible nursing concern: Respiratory status change requiring reassessment and communication.
Appropriate student action: Assess the patient, verify probe placement and signal, document SpO2 and respiratory assessment, and notify the nurse/instructor/preceptor according to policy.
Example 4: Pain With Elevated Blood Pressure and Pulse
Scenario: A patient reports severe pain before ambulation.
Objective vital sign cues: Pulse and blood pressure higher than earlier readings.
Subjective patient cues: Pain 8/10, sharp, at incision site.
Other assessment cues: Guarding, tense posture.
Possible nursing concern: Pain affecting function and physiologic response.
Appropriate student action: Assess pain fully, document pain score and vital signs, communicate findings according to policy, and follow instructor/preceptor guidance.
When to Report Vital Signs
Nursing students should report vital signs according to facility parameters, instructor/preceptor guidance, provider orders, early warning systems if used, and patient condition.
Report or seek guidance when:
- A reading is outside assigned parameters
- A value changes suddenly
- A trend is worsening
- The patient has concerning symptoms
- The reading does not match the patient’s appearance
- The monitor reading seems unreliable but concerning
- The patient reports dizziness, shortness of breath, severe pain, weakness, or feeling faint
- You are unsure what the reading means
Do not guess. Escalate uncertainty. Students are not expected to manage concerning changes independently. They are expected to reassess, document, communicate, and follow policy.
How to Study Vital Signs for Nursing School
To study vital signs well, learn the numbers and the nursing thinking behind them.
Use this approach:
- Learn common adult ranges first.
- Study pediatric and newborn ranges separately.
- Memorize what each vital sign measures.
- Practice manual blood pressure and pulse assessment.
- Count respirations accurately.
- Learn factors affecting each reading.
- Practice documentation examples.
- Compare one-time readings with trends.
- Use case scenarios to cluster cues.
- Review common technique errors.
- Ask instructors to clarify facility-specific parameters.
Strong students do not simply ask, “Is this number normal?” They ask, “Is this number expected for this patient, at this time, with these symptoms, using this technique?”
When to Ask for Help With Vital Signs Assignments
Students may need help with vital signs assignments, nursing assessment questions, case studies, care plans, clinical reflections, documentation examples, or interpretation of abnormal findings.
Academic support can help students organize answers, explain cue clustering, apply nursing assessment concepts, and write clearer clinical reasoning. If you are working on an assignment, you may find support through nursing assignment help , nursing case study help, or healthcare assignment help.
Use academic help to understand nursing concepts and improve your writing, not to replace clinical judgment, facility policy, instructor feedback, or patient-specific guidance.
FAQs About Vital Signs
1. What are the five main vital signs?
The five main vital signs commonly taught in nursing are temperature, pulse, respiratory rate, blood pressure, and oxygen saturation. Pain is often assessed alongside vital signs in many settings, but it is subjective and should be documented using the appropriate pain assessment tool.
2. What are normal vital signs for adults?
Common adult learning ranges include temperature around 36.5°C–37.3°C, pulse 60–100 bpm, respirations about 12–20 breaths/minute, and blood pressure often discussed around 90/60 to below 120/80 mmHg in general references. These ranges vary by source, institution, patient condition, baseline, and measurement method.
3. Are pediatric vital signs different from adult vital signs?
Yes. Pediatric vital signs differ by age. Younger children often have higher heart rates and respiratory rates than adults. Nursing students should use age-specific references and avoid applying adult ranges to infants, toddlers, preschoolers, school-age children, or adolescents.
4. What are newborn vital signs?
Newborn vital signs include temperature, heart rate, respiratory rate, and other newborn-specific observations such as color, tone, feeding behavior, and adaptation after birth. Newborns require specific assessment guidance because their thermoregulation and respiratory transition differ from older children and adults.
5. What are orthostatic vital signs?
Orthostatic vital signs assess changes in blood pressure and pulse with position changes, such as lying, sitting, and standing, depending on policy. They may be used when dizziness, falls risk, dehydration, blood loss, medication effects, or autonomic concerns are relevant.
6. Is pain considered a vital sign?
Pain is commonly assessed with vital signs in many clinical settings, but it is not objective like temperature or blood pressure. Pain is subjective and should be assessed using appropriate patient-centered tools. Normal vital signs do not mean pain is absent.
7. What can affect vital signs?
Vital signs can be affected by age, activity, pain, anxiety, fever, medications, hydration, posture, oxygen therapy, chronic conditions, environment, recent procedures, sleep, caffeine, nicotine, and measurement technique.
8. Why should nurses compare vital signs with baseline?
Baseline comparison helps nurses recognize meaningful changes. A value may be technically within a normal range but still concerning if it is far from the patient’s usual pattern or part of a worsening trend.
9. How should vital signs be documented?
Document the value, unit, time, route or site, patient position if relevant, oxygen device if applicable, pain score if required, reassessment, and communication according to facility policy. Use precise entries such as “BP 118/72 mmHg, right arm, sitting, automated cuff.”
10. When should nursing students report abnormal vital signs?
Students should report abnormal or concerning vital signs according to facility policy, instructor or preceptor guidance, provider orders, early warning systems if used, and patient condition. Report sudden changes, worsening trends, values outside assigned parameters, symptoms, or readings that do not match the patient’s presentation.
Final Thoughts on Vital Signs
Vital signs are essential nursing assessment data, but normal ranges are only a starting point. Nursing students must learn accurate measurement, careful documentation, trend recognition, cue clustering, reassessment, and appropriate reporting.
Temperature, pulse, respiratory rate, blood pressure, oxygen saturation, and pain assessment each provide important clues. However, no single number tells the whole story. Patient baseline, symptoms, age, clinical condition, measurement technique, device accuracy, and facility guidance all matter.
If students need help with vital signs assignments, nursing assessment case studies, clinical reflection, documentation examples, or care plan interpretation, they can upload their instructions and rubric for academic guidance.
References
Ernstmeyer, K., & Christman, E. (Eds.). (2023). Nursing skills. Open RN. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/
Ernstmeyer, K., & Christman, E. (Eds.). (2025). Nursing health promotion: Table 12.5c, normal newborn vital signs. Open RN. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/
MedlinePlus. (2025). Vital signs. U.S. National Library of Medicine. https://medlineplus.gov/ency/article/002341.htm
OpenStax. (2024). Fundamentals of nursing: How to perform vital signs. Rice University. https://openstax.org/books/fundamentals-nursing/pages/7-2-how-to-perform-vital-signs
Reuter-Sandquist, M., Ernstmeyer, K., & Christman, E. (2022). Nursing assistant: A nursing process approach. Open RN. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/
Royal Children’s Hospital Melbourne. (n.d.). Acceptable ranges for physiological variables. https://www.rch.org.au/clinicalguide/guideline_index/normal_ranges_for_physiological_variables/
Sapra, A., Malik, A., & Bhandari, P. (2023). Vital sign assessment. StatPearls. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK553213/
U.S. Food and Drug Administration. (2025). Pulse oximeter basics. https://www.fda.gov/consumers/consumer-updates/pulse-oximeter-basics