Pediatric dosage calculations can feel challenging when nursing students move from basic adult dosage math to weight-based pediatric medication problems. Many students can solve “desired over have” questions, but become unsure when the question includes kilograms, mg/kg, mg/kg/day, divided doses, liquid concentrations, safe dose range checks, or strict rounding rules.
This guide explains pediatric kg conversion, weight-based formulas, mg/kg and mg/kg/day calculations, divided doses, pediatric liquid medication math, reconstitution basics, IV math examples, body surface area basics, rounding safety, common mistakes, and worked practice problems.
This guide is for nursing education and pediatric dosage calculation practice only. Pediatric medication administration must follow provider orders, medication labels, approved pediatric drug references, facility policy, instructor guidance, and scope of practice.
If you need a broader review of formulas, unit conversions, oral medications, IV rates, reconstitution, rounding, and general nursing math, start with our full guide on dosage calculations for nursing students. This article stays focused on pediatric dosage calculations so you can go deeper into child-specific medication math.
Pediatric medication safety requires more than arithmetic. Nurses must verify the order, patient identity, current weight, route, frequency, allergies, drug reference information, decimal placement, measuring device, and required double-checks before medication administration. Medication errors can occur at several points in the medication-use process, and pediatric patients are especially vulnerable when calculations, weights, or decimals are handled poorly (D’Errico et al., 2022; Tariq et al., 2024).
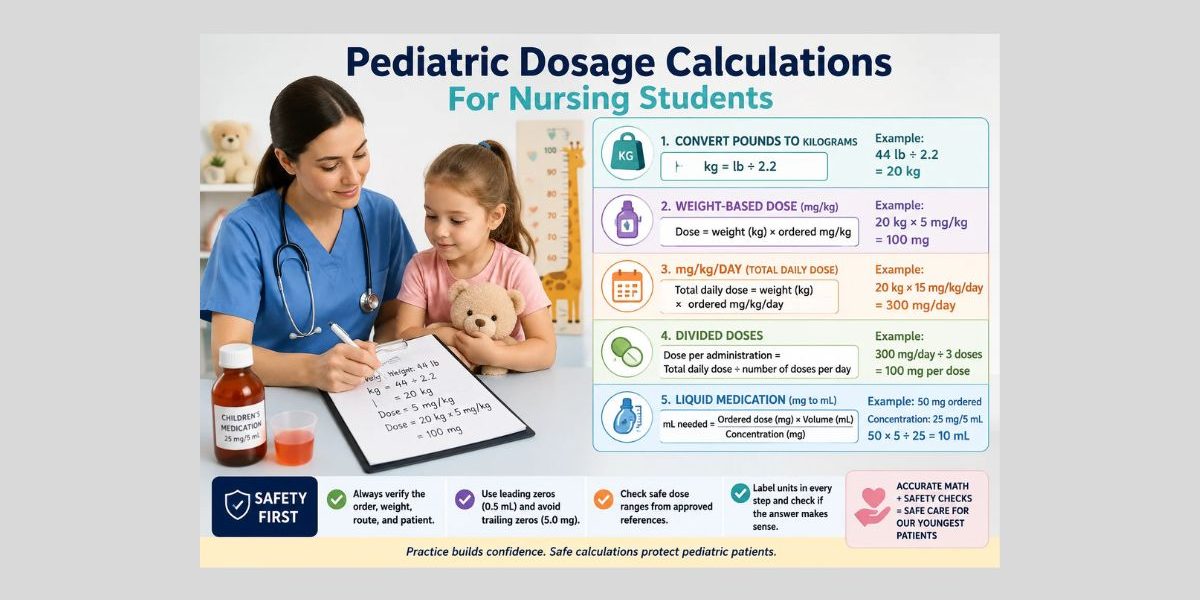
Quick Answer: What Are Pediatric Dosage Calculations?
- Pediatric dosage calculations are nursing math methods used to calculate or verify medication doses for children based on weight, ordered dose, available concentration, frequency, and safe dose range information.
- Many pediatric examples use kg, mg/kg, mg/kg/day, divided doses, liquid concentrations, or safe dose checks.
- Pediatric calculations require careful unit conversion, especially pounds to kilograms.
- Safe dose range checks must come from approved drug references, instructor examples, or facility policy.
- A correct calculation does not replace medication safety checks, provider orders, pediatric drug references, or supervision.
- Nursing students should show every step, label units, avoid unsafe decimals, and check whether the answer is reasonable.
What Makes Pediatric Dosage Calculations Different?
Pediatric dosage calculations differ from many adult dosage calculations because children often receive doses based on weight. A child’s weight, age, formulation, route, frequency, and prescribed concentration may affect how a calculation is set up. Children are not simply small adults, so nursing students must avoid guessing or scaling doses casually.
Small calculation errors can matter more in pediatrics because the therapeutic margin may be narrower, the child’s body size is smaller, and liquid medication amounts may be measured in small volumes. Pediatric medication errors are widely recognized as a major safety concern, especially when weight-based dosing, decimal placement, unclear orders, or communication gaps are involved (D’Errico et al., 2022).
A correct math answer is only one part of safe medication practice. Students must still verify the order, route, time, patient identity, allergies, medication label, safe range, drug reference, and facility or instructor requirements. Medication administration education often emphasizes rights of medication administration and the nurse’s responsibility to check orders and medications carefully before administration (Hanson & Haddad, 2023).
Pediatric Dosage Calculation Formula: Core Methods
Pediatric dosage calculations for nursing students may use more than one setup method. Your school may prefer desired over have, dimensional analysis, ratio and proportion, or a combination of methods. OpenStax explains that nursing dosage calculations commonly use basic formula, ratio and proportion, and dimensional analysis approaches (OpenStax, 2024).
| Method | How it helps in pediatric examples | Common pediatric mistake |
|---|---|---|
| Desired over have | Helps convert an ordered mg dose into mL when a liquid concentration is given | Using the total daily dose instead of the dose per administration |
| Dimensional analysis | Helps cancel units step by step, especially kg, mg, mL, and day | Forgetting to convert lb to kg before multiplying by mg/kg |
| Ratio and proportion | Helps compare equivalent dose and volume relationships | Misreading mg/5 mL as mg/mL |
The method matters less than safe setup. You should write the units, identify the final unit, and check whether the order asks for mg, mL, mL/hr, dose per day, or dose per administration.
Converting Pounds to Kilograms for Pediatric Dosage Calculations
Pediatric calculations often require weight in kilograms. If the child’s weight is given in pounds, convert it before using mg/kg or mg/kg/day.
Formula:
kg = lb ÷ 2.2
Current weight is important because many medication prescriptions for children and adults require weight to determine a safe and effective dose (Lubsch, 2023). In nursing math problems, use the weight provided in the question. In clinical settings, follow facility policy for obtaining and verifying current weight.
Example 1: Convert pounds to kilograms
Problem: A child weighs 44 lb. Convert to kg.
Setup:
44 lb ÷ 2.2 = 20 kg
Answer:
The child weighs 20 kg.
Example 2: Convert kilograms to pounds
Problem: A child weighs 18 kg. Convert to lb.
Setup:
18 kg × 2.2 = 39.6 lb
Answer:
The child weighs 39.6 lb.
Example 3: Why rounding too early can change the answer
Problem: A child weighs 33 lb. The fictional ordered dose is 6 mg/kg. Calculate the dose.
Step 1: Convert weight.
33 lb ÷ 2.2 = 15 kg
Step 2: Calculate dose.
15 kg × 6 mg/kg = 90 mg
Answer:
The dose is 90 mg.
Now imagine a student rounded a more precise weight too early in a different problem. If a child weighs 35 lb:
35 lb ÷ 2.2 = 15.9 kg
If rounded to 16 kg before calculating:
16 kg × 6 mg/kg = 96 mg
If kept as 15.9 kg:
15.9 kg × 6 mg/kg = 95.4 mg
The difference may look small, but pediatric rounding rules matter. Follow instructor, medication, measuring device, and facility requirements.
Weight-Based Pediatric Dose Calculation: mg/kg
The mg/kg dosage calculation means milligrams of medication per kilogram of body weight.
Basic formula:
Dose = weight in kg × ordered mg/kg
Example 1: Single-dose mg/kg calculation
Problem: A fictional pediatric order says Medication A is ordered at 4 mg/kg for one dose. The child weighs 12 kg. How many mg are ordered?
Setup:
12 kg × 4 mg/kg = 48 mg
Answer:
The ordered dose is 48 mg.
Reasonableness check:
The final unit is mg, and kg cancels out. That matches the question.
Example 2: Weight-based dose with liquid concentration
Problem: Medication A is ordered at 5 mg/kg. The child weighs 10 kg. The available liquid concentration is 25 mg/5 mL. How many mL are needed?
Step 1: Calculate ordered mg.
10 kg × 5 mg/kg = 50 mg
Step 2: Convert mg to mL.
25 mg = 5 mL
50 mg = x mL
50 mg × 5 mL ÷ 25 mg = 10 mL
Answer:
Give 10 mL in this fictional education-only problem.
Safety check:
In real practice, students must verify the provider order, medication label, route, frequency, safe range, measuring device, and supervision requirements.
Example 3: Instructor rounding rule stated
Problem: Medication A is ordered at 3.5 mg/kg. The child weighs 18.2 kg. The instructor says to round the final mg answer to the nearest tenth. Calculate the dose.
Setup:
18.2 kg × 3.5 mg/kg = 63.7 mg
Answer:
The dose is 63.7 mg.
Rounding note:
The final answer is already at the nearest tenth. Do not round the weight before multiplying unless instructed.
Pediatric mg/kg/day Calculations
The mg/kg/day calculation means the total daily dose is based on the child’s weight. Students must identify whether the question asks for the total daily dose or the amount per administration.
Formula:
Total daily dose = weight in kg × ordered mg/kg/day
Example 1: Total daily dose
Problem: A fictional order is 12 mg/kg/day. The child weighs 14 kg. What is the total daily dose?
Setup:
14 kg × 12 mg/kg/day = 168 mg/day
Answer:
The total daily dose is 168 mg/day.
Example 2: Daily dose divided into ordered doses
Problem: Medication A is ordered at 20 mg/kg/day divided into 4 equal doses. The child weighs 16 kg. How many mg should be given per dose?
Step 1: Calculate total daily dose.
16 kg × 20 mg/kg/day = 320 mg/day
Step 2: Divide by number of doses.
320 mg/day ÷ 4 doses/day = 80 mg/dose
Answer:
Each dose is 80 mg.
Common error:
Do not give 320 mg as one administration if the order says divided into 4 doses.
Divided Dose Calculations in Pediatrics
Divided dose calculation means separating a total daily amount into the number of doses ordered per day. This is one of the most common areas where pediatric nursing dosage calculations become confusing.
| Wording in question | What it means | Common mistake |
|---|---|---|
| mg/kg/dose | Calculate each dose directly | Treating it as a total daily dose |
| mg/kg/day | Calculate the total daily dose | Forgetting to divide by frequency |
| Divided every 6 hours | Usually 4 doses in 24 hours | Dividing by 6 instead of 4 |
| Divided BID | 2 doses per day | Giving the whole daily dose at once |
| Divided TID | 3 doses per day | Confusing TID with every 3 hours |
Example 1: Divided BID
Problem: Medication A is ordered at 18 mg/kg/day divided BID. The child weighs 11 kg. Calculate mg per dose.
Step 1: Total daily dose.
11 kg × 18 mg/kg/day = 198 mg/day
Step 2: BID means 2 doses per day.
198 mg/day ÷ 2 = 99 mg/dose
Answer:
The child receives 99 mg per dose in this fictional example.
Example 2: Divided every 8 hours
Problem: Medication A is ordered at 30 mg/kg/day divided every 8 hours. The child weighs 20 kg. Calculate mg per dose.
Step 1: Total daily dose.
20 kg × 30 mg/kg/day = 600 mg/day
Step 2: Every 8 hours means 3 doses in 24 hours.
600 mg/day ÷ 3 = 200 mg/dose
Answer:
Each dose is 200 mg.
Pediatric Safe Dose Range Calculations
Safe dose range pediatric calculations help students decide whether an ordered dose appears within an example reference range. In real practice, safe ranges must come from approved pediatric drug references, facility policy, instructor-provided examples, or pharmacist/provider clarification.
The fictional ranges below are for calculation practice only. They are not real pediatric dosing recommendations.
Example 1: Safe range per day
Problem: A fictional practice-only reference range for Medication A is 10–20 mg/kg/day. A child weighs 15 kg. The order is 240 mg/day. Is the order within the example range?
Step 1: Calculate minimum daily dose.
15 kg × 10 mg/kg/day = 150 mg/day
Step 2: Calculate maximum daily dose.
15 kg × 20 mg/kg/day = 300 mg/day
Step 3: Compare ordered dose.
Ordered dose = 240 mg/day
Range = 150–300 mg/day
Answer:
The order appears within the fictional practice-only range.
Safety note:
Real clinical decisions require approved pediatric references, medication labels, policy, and supervision.
Example 2: Safe range per dose
Problem: A fictional practice-only reference range for Medication A is 2–5 mg/kg/dose. A child weighs 18 kg. The ordered dose is 100 mg per dose. Is it within the example range?
Step 1: Minimum per dose.
18 kg × 2 mg/kg/dose = 36 mg/dose
Step 2: Maximum per dose.
18 kg × 5 mg/kg/dose = 90 mg/dose
Step 3: Compare.
Ordered dose = 100 mg/dose
Range = 36–90 mg/dose
Answer:
The ordered dose appears above the fictional practice-only range.
Safety note:
A student should not independently change or reject a real order. The correct action is to stop, verify the calculation, check approved references, and seek instructor, preceptor, pharmacist, or provider clarification.
Pediatric Liquid Medication Calculations
Pediatric medications are often supplied as liquids. The label may show mg/mL or mg/5 mL. Students must identify the ordered dose, available concentration, and final answer unit.
If the final answer is in mL, the measuring device matters. Pediatric medication safety resources often warn that liquid medicines and measuring devices can contribute to dosing confusion when volume or concentration is misunderstood (Institute for Quality and Efficiency in Health Care, 2025).
Example 1: mg/5 mL
Problem: Medication A is ordered at 60 mg. The available concentration is 30 mg/5 mL. How many mL are needed?
Setup:
60 mg × 5 mL ÷ 30 mg = 10 mL
Answer:
The dose volume is 10 mL.
Example 2: mg/mL
Problem: Medication A is ordered at 45 mg. The concentration is 15 mg/mL. How many mL are needed?
Setup:
45 mg ÷ 15 mg/mL = 3 mL
Answer:
The dose volume is 3 mL.
Example 3: Weight-based dose converted to mL
Problem: Medication A is ordered at 6 mg/kg. The child weighs 9 kg. The liquid concentration is 18 mg/3 mL. How many mL are needed?
Step 1: Calculate ordered mg.
9 kg × 6 mg/kg = 54 mg
Step 2: Convert mg to mL.
54 mg × 3 mL ÷ 18 mg = 9 mL
Answer:
The dose volume is 9 mL.
Pediatric Reconstitution Calculation Basics
Reconstitution examples involve using the final concentration after diluent is added. This article does not teach real medication preparation procedures. In clinical settings, students must follow the medication label, instructor instructions, facility policy, and scope of practice.
Fictional worked example
Problem: After reconstitution, Medication A has a final concentration of 100 mg/4 mL. The ordered dose is 75 mg. How many mL are needed?
Setup:
75 mg × 4 mL ÷ 100 mg = 3 mL
Answer:
The volume is 3 mL.
Safety check:
Use the final concentration stated in the question. Do not assume the concentration before or after reconstitution.
Pediatric IV Calculation Examples: Math Only
Pediatric IV calculations require strict policy, pump safety, supervision, and approved clinical guidance. This section is for math practice only. It does not teach IV insertion, pump programming, titration, compatibility, monitoring, or high-alert infusion procedures.
Basic formula:
mL/hr = total volume ÷ time in hours
Example 1: Basic mL/hr
Problem: A fictional IV fluid order says to infuse 120 mL over 6 hours. Calculate mL/hr.
Setup:
120 mL ÷ 6 hr = 20 mL/hr
Answer:
The rate is 20 mL/hr.
Example 2: Smaller pediatric volume
Problem: A fictional order says to infuse 75 mL over 5 hours. Calculate mL/hr.
Setup:
75 mL ÷ 5 hr = 15 mL/hr
Answer:
The rate is 15 mL/hr.
Body Surface Area Pediatric Dosage Calculations: Basic Overview
Body surface area dosage calculation may appear in advanced pediatric coursework or specialized contexts. BSA relates medication dosing to estimated body surface area rather than weight alone. However, BSA-based dosing is specialized and must follow approved references, institutional guidance, and instructor requirements.
This article does not provide oncology, chemotherapy, or high-alert medication examples. If your assignment includes BSA, use the exact formula, chart, nomogram, or calculator your instructor provides.
Pediatric Rounding Rules and Decimal Safety
Pediatric rounding rules depend on the medication, route, measuring device, school policy, and facility policy. Do not round intermediate steps too early unless instructed. Keep units visible through the full calculation.
Decimal safety is especially important. ISMP warns against trailing zeros and missing leading zeros because they can cause serious dose misinterpretation. For example, write 0.5 mL, not .5 mL. Write 5 mg, not 5.0 mg (Institute for Safe Medication Practices, 2024).
The Nursing Skills text in NCBI Bookshelf also teaches two important decimal standards: use leading zeros for doses below one whole unit and avoid trailing zeros after whole numbers (Ernstmeyer & Christman, 2021).
Examples:
- Correct: 0.5 mL
- Unsafe: .5 mL
- Correct: 5 mg
- Unsafe: 5.0 mg
- Safer habit: keep 15.9 kg during the calculation, then round the final answer as instructed
- Safer habit: label every answer as mg, mL, mg/day, mg/dose, or mL/hr
How to Check Whether a Pediatric Dosage Calculation Answer Makes Sense
Before accepting an answer, ask:
- Did I convert pounds to kilograms?
- Did I use mg/kg or mg/kg/day correctly?
- Does the question ask for total daily dose or dose per administration?
- Did I compare a daily order to a daily safe range, or a per-dose order to a per-dose range?
- Did I read mg/mL and mg/5 mL correctly?
- Is the final unit what the question asked for?
- Did I avoid unsafe decimals?
- Did I keep units visible?
- Does the mL amount make sense for the concentration?
- Should I repeat the calculation using another method?
In real clinical practice, students should seek instructor, preceptor, nurse, pharmacist, provider, or approved drug-reference verification when needed. Calculation accuracy does not replace medication administration safety checks.
You can also review medication administration routes to understand why route context matters, but remember that route knowledge does not replace medication order verification.
Common Pediatric Dosage Calculation Mistakes
| Mistake | Why it is risky | Safer habit |
|---|---|---|
| Using pounds instead of kilograms | Produces a much larger dose | Convert lb to kg first |
| Rounding weight too early | Can change pediatric dose | Keep decimals until final rounding |
| Confusing mg/kg with mg/kg/day | Mixes per-dose and daily dosing | Circle “per dose” or “per day” |
| Giving total daily dose as one dose | May create an unsafe administration amount | Divide by frequency when ordered |
| Misreading mg/mL and mg/5 mL | Produces wrong mL amount | Write the concentration as a fraction |
| Comparing daily dose to per-dose range | Leads to wrong safe-range conclusion | Match the order to the range wording |
| Using trailing zeros | May cause tenfold errors | Write 5 mg, not 5.0 mg |
| Missing leading zeros | May cause tenfold errors | Write 0.5 mL, not .5 mL |
| Omitting units | Makes the answer unclear | Label every step |
| Assuming math equals safety | Ignores clinical verification | Check order, label, policy, and reference |
Pediatric pharmacology also involves how a child’s body handles and responds to medication. For background, students can review pharmacokinetics for nursing students and pharmacodynamics for nursing students, but calculation practice should remain separate from prescribing decisions.
Pediatric Dosage Calculation Practice Problems With Worked Answers
The following pediatric dosage calculation practice problems use fictional education-only data. They are not clinical dosing recommendations.
Problem 1: lb to kg conversion
Problem: A child weighs 55 lb. Convert to kg.
Setup:
55 lb ÷ 2.2 = 25 kg
Final answer:
25 kg
Check:
The answer is in kg, which is needed for weight-based calculations.
Problem 2: mg/kg single dose
Problem: Medication A is ordered at 4 mg/kg. The child weighs 13 kg. Calculate the dose.
Setup:
13 kg × 4 mg/kg = 52 mg
Final answer:
52 mg
Check:
Kg cancels out, leaving mg.
Problem 3: mg/kg/day total daily dose
Problem: Medication A is ordered at 15 mg/kg/day. The child weighs 22 kg. Calculate the total daily dose.
Setup:
22 kg × 15 mg/kg/day = 330 mg/day
Final answer:
330 mg/day
Check:
The answer is total daily dose, not dose per administration.
Problem 4: Divided dose
Problem: Medication A is ordered at 24 mg/kg/day divided TID. The child weighs 10 kg. Calculate mg per dose.
Step 1:
10 kg × 24 mg/kg/day = 240 mg/day
Step 2:
240 mg/day ÷ 3 doses/day = 80 mg/dose
Final answer:
80 mg per dose
Check:
TID means three doses per day in this practice problem.
Problem 5: Safe dose range per day
Problem: A fictional practice-only range is 8–12 mg/kg/day. A child weighs 18 kg. The order is 190 mg/day. Is it within range?
Minimum:
18 kg × 8 mg/kg/day = 144 mg/day
Maximum:
18 kg × 12 mg/kg/day = 216 mg/day
Compare:
190 mg/day falls between 144 and 216 mg/day.
Final answer:
The order appears within the fictional practice-only range.
Check:
The range and order are both daily amounts.
Problem 6: Safe dose range per dose
Problem: A fictional practice-only range is 1.5–3 mg/kg/dose. A child weighs 20 kg. The order is 70 mg per dose. Is it within range?
Minimum:
20 kg × 1.5 mg/kg/dose = 30 mg/dose
Maximum:
20 kg × 3 mg/kg/dose = 60 mg/dose
Compare:
70 mg per dose is above 60 mg per dose.
Final answer:
The order appears above the fictional practice-only range.
Check:
A student should verify the math and seek instructor or clinical clarification in real settings.
Problem 7: Liquid medication calculation
Problem: Medication A is ordered at 90 mg. The available concentration is 45 mg/5 mL. Calculate mL.
Setup:
90 mg × 5 mL ÷ 45 mg = 10 mL
Final answer:
10 mL
Check:
The final answer is in mL, as requested.
Problem 8: Basic mL/hr calculation
Problem: A fictional IV order says to infuse 180 mL over 9 hours. Calculate mL/hr.
Setup:
180 mL ÷ 9 hr = 20 mL/hr
Final answer:
20 mL/hr
Check:
This is math-only practice. Real pediatric IV administration requires policy, pump safety, supervision, and approved clinical guidance.
What Our Pediatric Dosage Calculation Support Does Not Include
Academic support for pediatric medication math does not provide pediatric prescribing advice. It does not replace instructors, preceptors, pharmacists, providers, facility policies, or approved drug references.
It does not include:
- Fabricating patient weights, observations, labs, or medication data
- Inventing real safe dose ranges
- Adjusting real pediatric medication orders
- Recommending treatment
- Completing prohibited exams or practical assessments
- Providing high-alert medication protocols
- Replacing clinical supervision
The goal is to help students understand the calculation process, show work clearly, and learn safer reasoning habits.
How to Study Pediatric Dosage Calculations
Start with kg conversion. If you cannot convert pounds to kilograms confidently, mg/kg and mg/kg/day problems become harder.
Then practice identifying the wording. Circle mg/kg, mg/kg/day, per dose, per day, divided BID, divided TID, every 6 hours, every 8 hours, and total daily dose. Most errors happen before the arithmetic begins.
Use these study habits:
- Write units on every step.
- Convert lb to kg first.
- Keep extra decimals until the final step.
- Separate total daily dose from dose per administration.
- Practice safe dose range checks separately.
- Redo missed problems and name the error type.
- Check decimal placement before writing the final answer.
- Use leading zeros and avoid trailing zeros.
- Never guess in clinical practice.
If your difficulty is part of a larger class assignment, our nursing assignment help service can help you understand the instructions, organize your work, and practice step-by-step reasoning.
When to Ask for Help With Pediatric Dosage Calculations
Ask for help if you repeatedly miss kg conversion, mg/kg/day setup, divided doses, safe ranges, liquid concentrations, reconstitution examples, rounding, or pediatric IV math questions.
You may also need support if your instructor requires you to show a specific method, such as dimensional analysis, and you understand the answer but not the setup. Academic guidance can help you review practice questions, explain errors, and prepare for medication math coursework. For broader coursework support, you can also use our nursing homework help page.
FAQs About Pediatric Dosage Calculations
1. What are pediatric dosage calculations?
Pediatric dosage calculations are nursing math calculations used to determine or verify medication amounts for children. They often involve weight in kilograms, mg/kg, mg/kg/day, divided doses, liquid concentrations, and safe dose range checks.
2. Why are pediatric dosage calculations different from adult calculations?
They often rely on weight-based dosing, smaller dose volumes, stricter rounding, and careful safe-range checks. Pediatric patients are not simply small adults, so students must follow approved references, instructor guidance, and facility policy.
3. How do you convert pounds to kilograms for pediatric dosage calculations?
Divide pounds by 2.2.
Example:
44 lb ÷ 2.2 = 20 kg
4. What is the mg/kg pediatric dosage formula?
The basic formula is:
Dose = weight in kg × ordered mg/kg
Example:
12 kg × 4 mg/kg = 48 mg
5. What is the difference between mg/kg and mg/kg/day?
mg/kg usually refers to a dose based on body weight for one administration, depending on the question. mg/kg/day refers to the total daily dose based on body weight. If the daily dose is divided, you must divide by the number of doses per day.
6. How do divided doses work in pediatric calculations?
First calculate the total daily dose. Then divide by the ordered frequency. For example, if a daily dose is divided BID, divide by 2. If it is divided TID, divide by 3.
7. How do you check a pediatric safe dose range?
Use the approved or instructor-provided range. Multiply the child’s weight in kg by the minimum and maximum range. Then compare the ordered amount to the correct range, making sure you compare per-day values with per-day ranges and per-dose values with per-dose ranges.
8. How do you calculate pediatric liquid medication doses?
Calculate the ordered mg first if needed. Then use the concentration to convert mg to mL. For example, if the order is 60 mg and the concentration is 30 mg/5 mL:
60 mg × 5 mL ÷ 30 mg = 10 mL
9. What rounding rules matter in pediatric dosage calculations?
Follow instructor, medication, route, measuring device, and facility rules. Avoid rounding too early. Use leading zeros, such as 0.5 mL, and avoid trailing zeros, such as 5.0 mg.
10. What is the best way to practice pediatric dosage calculations?
Practice one skill at a time: kg conversion, mg/kg, mg/kg/day, divided doses, safe range checks, liquid medication calculations, and rounding. Show every step and review each missed problem by identifying the exact error.
Final Thoughts on Pediatric Dosage Calculations
Pediatric dosage calculations require careful weight conversion, unit setup, mg/kg and mg/kg/day interpretation, divided dose reasoning, safe dose range checks, liquid concentration math, and decimal safety. The goal is not speed alone. The goal is safe, accurate, reasoned calculation.
A correct calculation does not replace medication labels, provider orders, pediatric drug references, facility policy, instructor guidance, pharmacist clarification, or scope of practice. Students should slow down, label units, verify the wording, and check whether the final answer makes sense.
For a broader review of nursing math formulas and general calculation methods, use the full guide on broader dosage calculation methods.
If students need help understanding pediatric dosage calculation assignments, medication math practice, or nursing pharmacology coursework, they can upload their instructions, rubric, and practice questions for academic guidance.
References
D’Errico, S., Zanon, M., Radaelli, D., Padovano, M., Santurro, A., Scopetti, M., Frati, P., & Fineschi, V. (2022). Medication errors in pediatrics: Proposals to improve the quality and safety of care through clinical risk management. Frontiers in Medicine, 8, 814100. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8795662/
Ernstmeyer, K., & Christman, E. (Eds.). (2021). Nursing skills. Chippewa Valley Technical College. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK593207/
Hanson, A., & Haddad, L. M. (2023). Nursing rights of medication administration. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK560654/
Institute for Quality and Efficiency in Health Care. (2025). Medications for children: Getting the dose right. InformedHealth.org. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK361019/
Institute for Safe Medication Practices. (2024). ISMP list of error-prone abbreviations, symbols, and dose designations. https://online.ecri.org/hubfs/ISMP/Resources/ISMP_ErrorProneAbbreviation_List.pdf
Lubsch, L. (2023). Patient weight should be included on all medication prescriptions. Hospital Pharmacy, 58(6), 533–534. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10547047/
OpenStax. (2024). Pharmacology for nurses: Dosage calculations. Rice University. https://openstax.org/books/pharmacology/pages/2-4-dosage-calculations
Tariq, R. A., Vashisht, R., Sinha, A., & Scherbak, Y. (2024). Medication dispensing errors and prevention. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK519065/