Newborn vital signs require newborn-specific interpretation because early newborn assessment involves transition after birth, thermoregulation, respiratory adaptation, color, feeding, and activity.
Many nursing students learn adult vital signs first, then feel unsure when newborn values look very different. A newborn’s heart rate, respiratory rate, temperature stability, oxygen saturation context, skin color, tone, and feeding behavior must be interpreted together. Newborn vital signs are not simply “small adult” values or the same as older pediatric values.
This guide covers normal newborn vital signs, newborn temperature, heart rate, respiratory rate, oxygen saturation, blood pressure context, thermoregulation, respiratory transition, documentation, cue clustering, common mistakes, and when to report changes. This guide is for nursing education and newborn assessment learning only. Newborn vital sign assessment and response must follow facility policy, instructor guidance, provider orders, newborn condition, scope of practice, and clinical judgment.
Students who need the broader adult and general assessment overview can use the complete vital signs guide, which covers temperature, pulse, respiratory rate, blood pressure, oxygen saturation, pain assessment, measurement technique, documentation, trends, abnormal findings, and cue clustering. This supporting article stays focused on newborn vital signs and newborn-specific nursing assessment.
Quick Answer: What Are Newborn Vital Signs?
Newborn vital signs are measurable assessment data used to evaluate a newborn’s physiological status during the early newborn period.
They commonly include temperature, heart rate, and respiratory rate. Oxygen saturation may be monitored depending on screening, setting, timing, clinical condition, or facility policy. Blood pressure may be assessed depending on newborn acuity, provider order, unit policy, or clinical context.
Newborn values differ from adult and older pediatric values because newborns are adapting after birth.
Thermoregulation and respiratory transition are especially important in newborn assessment.
A single value should be interpreted with age in hours or days, gestational age, activity, feeding, color, respiratory effort, baseline, and facility guidance.
Nursing students should document values clearly and report concerning trends or cues according to policy.
What Makes Newborn Vital Signs Different?
Newborns are adapting from intrauterine to extrauterine life. This transition affects breathing, circulation, temperature control, oxygenation, feeding behavior, skin color, and activity. MedlinePlus explains that the newborn’s lungs are fluid-filled before birth and that major lung and circulatory changes occur once the newborn begins breathing after delivery (MedlinePlus, 2025).
Thermoregulation is also a major newborn concern. Newborns can lose heat more easily than older children or adults because of body size, limited reserves, wet skin after birth, environmental exposure, and immature temperature regulation. Newborns also rely heavily on nonshivering thermogenesis rather than mature shivering mechanisms, which makes temperature assessment more than a routine number (Elshazzly et al., 2023).
Newborn values differ from adult and older pediatric values. A newborn heart rate that appears very fast beside an adult range may be expected in the newborn period. A newborn respiratory pattern may be less regular than an adult pattern, so students need to count carefully and observe effort. The MSD Manual Professional Edition notes that neonatal respirations should be counted for a full minute because breathing can be irregular, and it lists a normal newborn respiratory rate of 40 to 60 breaths per minute (MSD Manual Professional Edition, 2023).
Newborn assessment also depends on age in hours or days, gestational age where relevant, sleep or awake state, crying, feeding, handling, environmental exposure, recent procedures, and clinical condition. Students should not interpret newborn vital signs by the numbers alone. Color, tone, respiratory effort, feeding behavior, perfusion, and overall appearance matter.
Newborn Vital Signs Chart
The chart below gives a practical nursing-student overview. Ranges may vary by source, gestational age, age in hours or days, birth condition, clinical setting, and facility policy. Use it as a learning guide, not as an absolute diagnostic rule.
| Vital sign | Common newborn reference range or assessment focus | Nursing note | Documentation reminder |
|---|---|---|---|
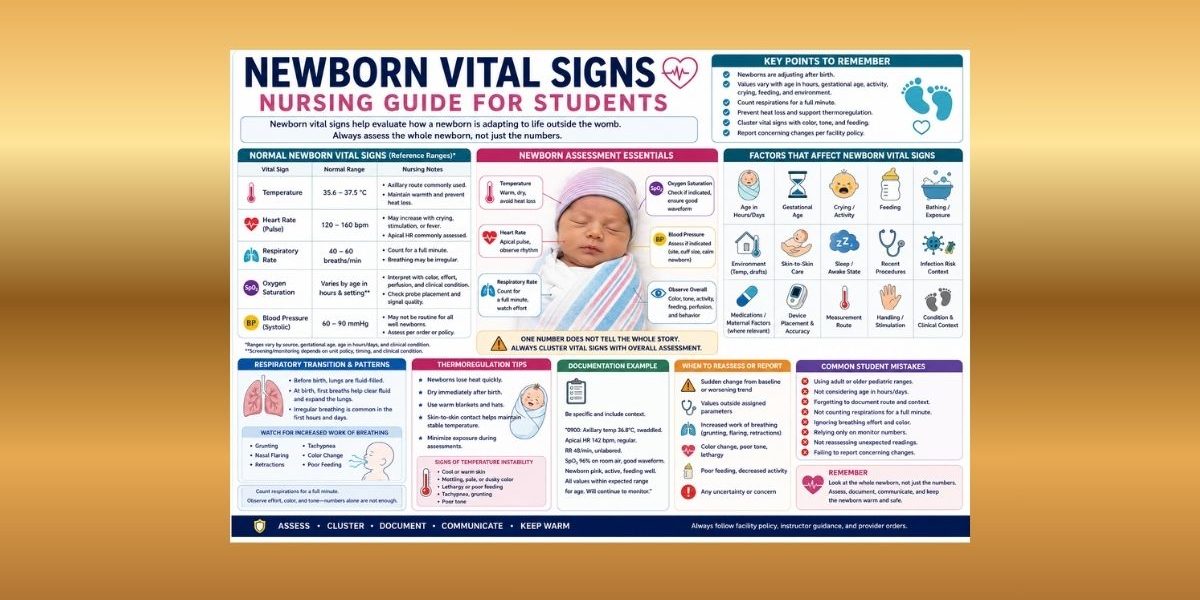
| Temperature | Commonly cited range around 35.6°C–37.5°C in one newborn reference table | Route and environment matter. Axillary temperature is commonly used in many newborn settings, but students must follow policy. | Document value, unit, route, time, and context such as swaddled, skin-to-skin, post-bath, or exposed. |
| Heart rate/pulse | Commonly cited newborn range 120–160 bpm | Heart rate may vary with sleep, crying, feeding, stimulation, temperature, and condition. | Document rate, method/site if required, rhythm if assessed, and newborn state. |
| Respiratory rate | Commonly cited range 40–60 breaths/min | Count for a full minute when required. Observe rhythm, effort, color, nasal flaring, grunting, and retractions. | Document rate, effort, pattern, oxygen context if applicable, and concerning cues. |
| Oxygen saturation context | Monitored depending on screening, setting, timing, policy, or condition | Interpret with respiratory effort, color, perfusion, activity, age after birth, and device signal quality. | Document percentage, room air or oxygen context if applicable, waveform/signal if relevant, and probe issues. |
| Blood pressure context | One newborn reference lists systolic BP 60–90 mmHg | May not be routine in all well-newborn settings. Depends on acuity, order, policy, or clinical indication. | If assessed, document reading, limb/site, cuff size or method if required, position, and context. |
A newborn vital signs table in NCBI Bookshelf lists heart rate 120–160 beats per minute, respiratory rate 40–60 breaths per minute, systolic blood pressure 60–90 mmHg, and temperature 35.6°C–37.5°C (OpenStax/NCBI Bookshelf, n.d.).
Newborn Temperature and Thermoregulation
Newborn temperature assessment is a major part of newborn nursing assessment because newborns can lose heat quickly. Temperature instability may be associated with environmental exposure, wet linens, bathing, delayed drying, inadequate covering, prolonged assessment exposure, infection risk context, respiratory effort, feeding difficulty, or other clinical factors. Students should not diagnose the cause from temperature alone.
Thermoregulation matters because newborns are adjusting to the outside environment. Elshazzly et al. (2023) explain that newborns use nonshivering thermogenesis and have unique heat-production demands related to breathing, feeding, and temperature maintenance.
Temperature route and measurement method matter. A temperature should never be documented without the route when route affects interpretation. A chart entry such as “36.8°C” is less complete than “36.8°C axillary at 0900; newborn swaddled.” Students should follow facility policy for route, timing, equipment, and reassessment.
Factors that may affect newborn temperature include:
- Environmental temperature
- Wet linens or skin exposure
- Bathing
- Skin-to-skin contact
- Warmer or incubator context where relevant
- Swaddling
- Feeding state
- Crying or activity
- Gestational age
- Infection risk context
- Timing after birth
- Measurement route
- Device accuracy
Do not use this article as a warming protocol. If a temperature is unexpected or concerning, reassess according to policy, maintain safety within student scope, and report to the nurse, instructor, preceptor, provider, or neonatal team as required.
Newborn Heart Rate and Pulse Assessment
Newborn heart rate differs from adult ranges. A heart rate of 120–160 bpm is commonly cited for newborns, while adult resting heart rate references are much lower. This difference reflects newborn physiology, including higher metabolic demands and adaptation to extrauterine life (Elshazzly et al., 2023).
Newborn heart rate may vary with sleep, crying, feeding, handling, stimulation, temperature, oxygenation context, and clinical condition. A newborn may have a different heart rate when asleep than when crying or being handled. Students should document context when it helps explain the reading.
Apical heart rate may be emphasized in newborn assessment depending on setting, instructor guidance, and facility policy. Newborn pulse quality, rhythm, color, tone, and perfusion cues may also provide context. A number alone does not tell the whole story.
For example, “Apical HR 142 bpm, regular, newborn asleep” is stronger documentation than “HR normal.” It tells the reader the rate, method, rhythm, and newborn state.
Students should also avoid using adult reasoning. A newborn heart rate that seems high compared with adult values may be expected. A value within a newborn range may still require attention if the newborn appears pale, poorly perfused, lethargic, distressed, or different from previous assessment.
Newborn Respiratory Rate and Breathing Patterns
Newborn respiratory assessment is especially important because newborns are transitioning to independent breathing after birth. The first breaths help clear lung fluid and support major circulatory changes (MedlinePlus, 2025).
A commonly cited newborn respiratory rate is 40–60 breaths per minute. The MSD Manual Professional Edition states that neonatal respirations should be counted over a full minute because neonatal breathing may be irregular, and it identifies grunting, nasal flaring, and retractions as signs of respiratory distress (MSD Manual Professional Edition, 2023).
Students should observe:
- Respiratory rate
- Rhythm and pattern
- Work of breathing
- Nasal flaring
- Grunting
- Retractions
- Chest symmetry
- Color
- Tone
- Feeding tolerance where relevant
- Oxygen saturation if monitored
- Overall newborn appearance
Some irregularity may occur in newborn breathing patterns, but students should not dismiss concerning signs. Increased work of breathing, color change, persistent grunting, retractions, poor tone, poor feeding, or a worsening trend requires reassessment and reporting according to facility guidance.
Documentation should include rate, effort, pattern, and oxygen context if applicable. For example: “RR 48/min, unlabored; no retractions noted” is clear and useful.
This section is not a respiratory treatment guide. Do not use it for oxygen administration, neonatal resuscitation, or emergency steps.
Newborn Oxygen Saturation and SpO2 Context
Newborn oxygen saturation, or newborn SpO2, may be monitored depending on setting, timing after birth, screening requirements, clinical condition, or facility policy. In some contexts, pulse oximetry is part of screening or observation. In others, routine continuous monitoring may not be used for every well newborn.
SpO2 should never be interpreted alone. It should be read with respiratory effort, color, perfusion, activity, age after birth, signal quality, and overall condition. Motion, crying, probe placement, low perfusion, skin factors, and device limitations can affect readings. StatPearls explains that pulse oximetry estimates oxygen saturation but should be interpreted with clinical status and awareness of device limitations (Torp et al., 2023).
Students should check whether the reading has a reliable signal before documenting an unexpected number. If the probe is loose, the newborn is moving, or the waveform is poor, the displayed value may not reflect the newborn’s true status. Repositioning and reassessment should follow facility policy and instructor guidance.
Documentation examples:
- “SpO2 96% with good waveform; probe repositioned before final reading.”
- “SpO2 documented per unit policy; newborn pink, unlabored respirations.”
- “SpO2 reading inconsistent with appearance; probe checked and RN notified per policy.”
Do not provide oxygen administration instructions. Oxygen support, device changes, and escalation must follow provider orders, newborn condition, scope of practice, and facility policy.
Newborn Blood Pressure: When It May Be Relevant
Newborn blood pressure may not be routine in all well-newborn settings. It may be assessed depending on acuity, provider order, facility policy, newborn condition, or clinical context. This is why blood pressure should be covered in a newborn vital signs guide, but it should not dominate the article.
When newborn blood pressure is assessed, technique matters. Cuff size, limb or site, movement, crying, newborn state, and device accuracy may affect the reading. A crying or moving newborn may produce a less reliable measurement. A cuff that does not fit correctly can distort the result.
One newborn vital signs table lists systolic blood pressure 60–90 mmHg as a normal newborn range, but students should avoid applying one number to every newborn without context (OpenStax/NCBI Bookshelf, n.d.).
Documentation should include the reading, site or limb, method if required, position if relevant, and context. Example: “BP 68/40 mmHg, right leg, newborn asleep, appropriate cuff per unit policy.”
Do not provide treatment advice for abnormal newborn blood pressure. Reassess technique, document accurately, and report according to policy.
Newborn Vital Signs vs Pediatric Vital Signs
Newborn vital signs are not the same as older pediatric vital signs. Newborns are in a unique transition period after birth, while older pediatric age groups are assessed according to developmental stage and age-based ranges.
| Area | Newborn focus | Older pediatric focus |
|---|---|---|
| Main context | Transition after birth, thermoregulation, respiratory adaptation | Age-based growth and developmental stage |
| Temperature | Heat loss prevention, route, environment, swaddling, skin-to-skin context | Fever, activity, route, illness context, developmental cooperation |
| Respiratory assessment | Transition, irregular pattern, effort, color, grunting, flaring, retractions | Rate by age, effort, symptoms, activity, ability to feed/play/speak |
| Heart rate | Higher newborn range, affected by sleep, crying, feeding, temperature | Age-based pulse ranges from infant through adolescent |
| Oxygen saturation | Screening/monitoring context, probe quality, transition timing | Respiratory condition, device quality, effort, oxygen context |
| Documentation | Newborn state, route, environmental context, feeding/activity, transition cues | Age, behavior, activity, symptoms, caregiver report, developmental context |
Do not merge newborn and pediatric ranges in assignments unless the rubric or source specifically does so. Newborns deserve separate attention because their physiology and assessment priorities differ from infants beyond the immediate newborn period.
Factors That Affect Newborn Vital Signs
| Factor | Vital signs affected | Newborn nursing consideration |
|---|---|---|
| Age in hours/days | Temperature, HR, RR, SpO2 context | Interpret with transition stage and unit policy |
| Gestational age | Temperature, HR, RR, feeding, tone | Consider maturity and facility guidance |
| Sleep/awake state | HR, RR, tone, activity | Document newborn state when relevant |
| Crying | HR, RR, SpO2 artifact | Reassess when calm if policy indicates |
| Feeding | HR, RR, temperature context, activity | Consider timing before interpreting changes |
| Bathing | Temperature | Document post-bath context if relevant |
| Environmental temperature | Temperature | Minimize unnecessary exposure according to policy |
| Skin-to-skin | Temperature, HR, RR, bonding context | Document if relevant to assessment |
| Handling/stimulation | HR, RR, crying, SpO2 artifact | Observe before and after handling when appropriate |
| Respiratory transition | RR, color, SpO2, effort | Assess effort, color, tone, and trend |
| Recent procedures | HR, RR, pain/stress cues | Cluster with behavior and condition |
| Medications/maternal factors where relevant | HR, RR, tone, feeding | Stay within student scope and report concerns |
| Infection risk context where relevant | Temperature, HR, RR, feeding, tone | Do not diagnose; report concerning cues |
| Measurement route | Temperature interpretation | Document route clearly |
| Device placement | SpO2, BP | Check probe/cuff placement before accepting unexpected readings |
| Perfusion | SpO2, color, capillary refill context | Interpret with color, warmth, and overall assessment |
| Facility policy | All vital signs | Follow unit-specific timing, ranges, and reporting rules |
MedlinePlus notes that newborn and infant heart rate, breathing, muscle tone, and body movements vary across sleep and activity states, and stress or stimulation can affect bodily functions (MedlinePlus, 2025).
Newborn Vital Sign Trends vs One-Time Readings
One newborn vital sign reading can be misleading. A newborn may cry during assessment, move during SpO2 monitoring, have temperature affected by exposure, or show a temporary change after feeding, bathing, or handling. Trends show whether the newborn is adapting, stable, or changing.
Students should compare each reading with previous readings and the newborn’s current condition. Ask:
- Is the newborn asleep, crying, feeding, or recently handled?
- What is the newborn’s age in hours or days?
- Is the newborn term or preterm where relevant?
- Is the newborn warm, pink, active, and feeding as expected?
- Is the respiratory effort unlabored?
- Is the reading consistent with previous values?
- Was the measurement technique reliable?
- Does the newborn’s appearance match the number?
A technically “normal” value may still matter if it conflicts with appearance or trend. For example, a respiratory rate within range may not be reassuring if the newborn has grunting or retractions. A temperature within range may still need follow-up if it is falling over time after repeated assessments.
Unexpected readings should be repeated according to policy. Concerning trends should be reported according to facility policy, instructor guidance, provider orders, and newborn condition.
How to Take Newborn Vital Signs Accurately
Accurate newborn vital signs require newborn-appropriate equipment, safe handling, and careful observation. Students should follow facility and instructor guidance rather than improvising.
Use this practical checklist:
- Confirm the newborn’s identity according to policy.
- Review the newborn’s age in hours or days.
- Consider gestational age where relevant.
- Use newborn-appropriate equipment.
- Minimize heat loss and unnecessary exposure.
- Observe color, breathing, tone, activity, and overall appearance before disturbing the newborn when appropriate.
- Consider timing around feeding, crying, bathing, and handling.
- Document temperature route.
- Count respirations carefully according to newborn assessment expectations.
- Check device placement and signal quality if using SpO2.
- Verify unexpected readings.
- Compare readings with previous values and the full newborn assessment.
- Report concerning findings according to policy.
This checklist supports learning. It does not replace skills-lab instruction, unit procedure, maternal-newborn policy, or neonatal team guidance.
Manual vs Automated Newborn Vital Signs
Automated devices may be used depending on setting, acuity, facility policy, and equipment availability. However, newborn monitoring can be affected by motion, crying, probe placement, cuff size, poor perfusion, and device error.
Manual or direct assessment skills remain important. Students need to observe the newborn, not just copy a device value. A monitor may show a number, but the newborn’s color, tone, respiratory effort, and behavior tell the student whether the number fits the full assessment.
Unexpected readings should be reassessed rather than copied without question. If the number does not match the newborn’s appearance, check technique and seek guidance.
Examples:
- A low SpO2 reading with a loose probe may need repositioning and reassessment.
- A high heart rate during crying may need interpretation with activity state.
- A temperature after prolonged exposure may need contextual documentation and reporting according to policy.
- A BP reading during movement may need verification if required.
Newborn Vital Signs Documentation
Newborn vital signs documentation should be specific, objective, and contextual. Avoid vague charting such as “newborn stable” without actual values when vital signs should be recorded.
Document:
- Value
- Unit
- Time
- Route, site, or method
- Newborn state if relevant
- Temperature context if relevant
- Oxygen context if applicable
- Feeding, crying, bathing, skin-to-skin, or handling context when relevant
- Reassessment where required
- Abnormal findings and who was notified according to policy
Examples:
“Temperature 36.8°C axillary at 0900; newborn swaddled.”
“Apical HR 142 bpm, regular, newborn asleep.”
“RR 48/min, unlabored; no retractions noted.”
“SpO2 96% with good waveform; probe repositioned before final reading.”
“Temperature repeated per policy after low initial reading; RN notified.”
“RR 62/min with mild nasal flaring observed; instructor and assigned RN notified.”
Clear documentation supports continuity, communication, and safe reassessment.
Abnormal Newborn Vital Signs: How Nursing Students Should Think
Abnormal newborn vital signs may mean a value is outside the expected range, changed from previous readings, inconsistent with newborn appearance, trending in a concerning direction, or associated with other cues. Students should not interpret one number alone.
Cluster cues:
- Temperature
- Heart rate
- Respiratory rate
- Oxygen saturation if monitored
- Respiratory effort
- Color
- Tone
- Feeding behavior
- Activity level
- Perfusion
- Age in hours or days
- Gestational age where relevant
- Environmental exposure
- Delivery or transition context within student scope
- Staff or caregiver observations
- Measurement technique
- Device accuracy
Example: Low Temperature With Environmental Exposure Context
A newborn temperature is lower than expected after bathing or exposure. This may be related to environmental factors, but the student should not assume. Reassess according to policy, document route and context, and report as required.
Example: Increased Respiratory Effort With Color Change
A newborn has a respiratory rate near the upper range but also shows retractions or color change. The “number” alone is not enough. Respiratory effort and color require prompt reporting according to facility guidance.
Example: Abnormal SpO2 Reading With Poor Probe Placement
A low SpO2 reading appears while the probe is loose and the newborn is moving. The reading may be artifact, but it must be checked. Assess the newborn, correct placement according to policy, reassess, and report if concerns continue.
Example: “Normal” Value but Newborn Appears Lethargic or Feeding Poorly
A heart rate or temperature may appear within range, but poor tone, lethargy, weak feeding, or color change can still be concerning. A normal value does not erase abnormal assessment cues.
Do not diagnose or give treatment instructions. Reassess technique, maintain safety within scope, document clearly, and report according to policy.
Newborn Vital Signs and Cue Clustering Examples
Example 1: Thermoregulation Concern
Scenario: A newborn has an axillary temperature lower than expected after being unswaddled for an assessment.
Objective vital sign cues: Temperature is below the expected range for the newborn reference used by the facility.
Newborn assessment cues: Newborn is quiet, skin feels cool, and extremities are exposed.
Caregiver/staff observations: Staff notes the newborn had a recent bath.
Possible nursing concern: The newborn may have temperature instability or environmental heat loss context, but the student should not diagnose the cause.
Appropriate student action: Follow facility policy, minimize unnecessary exposure within scope, reassess as directed, document route and context, and report to the assigned nurse, instructor, preceptor, provider, or neonatal team as required.
Example 2: Respiratory Effort Concern
Scenario: A newborn has RR 64/min with mild retractions.
Objective vital sign cues: Respiratory rate is above a commonly cited newborn range, and effort is increased.
Newborn assessment cues: Mild nasal flaring and retractions are present.
Caregiver/staff observations: Staff notes the newborn has been less interested in feeding.
Possible nursing concern: The cue cluster may suggest respiratory transition or respiratory compromise concerns, but the student should not diagnose.
Appropriate student action: Reassess according to policy, document rate and effort, maintain safety, and report promptly to the nurse, instructor, preceptor, provider, or neonatal team.
Example 3: Oxygen Saturation Reading Affected by Probe Placement
Scenario: SpO2 reads lower than expected, but the newborn is moving and the probe is loose.
Objective vital sign cues: Low displayed SpO2 with poor signal quality.
Newborn assessment cues: Newborn appears pink with unlabored respirations.
Caregiver/staff observations: Staff notes the probe has shifted.
Possible nursing concern: The reading may be inaccurate, but a true oxygenation concern must not be dismissed.
Appropriate student action: Check probe placement according to policy, reassess signal and newborn appearance, document the final reliable reading, and report persistent concerns.
Example 4: Feeding/Activity Context With Changed Vital Signs
Scenario: Heart rate and respiratory rate are higher after crying and feeding.
Objective vital sign cues: HR and RR are elevated compared with earlier readings.
Newborn assessment cues: Newborn is crying but calms after handling decreases.
Caregiver/staff observations: Caregiver reports the newborn was crying before feeding.
Possible nursing concern: Activity and crying may affect readings, but trends and appearance still matter.
Appropriate student action: Reassess when appropriate per policy, document newborn state, compare with previous values, and report if readings remain concerning or other cues appear.
Common Newborn Vital Signs Mistakes Nursing Students Make
| Mistake | Why it matters | Safer habit |
|---|---|---|
| Using adult ranges for newborns | Newborn HR and RR are normally different from adults | Use newborn-specific ranges and facility guidance |
| Using older pediatric ranges for newborns | Newborn transition is unique | Separate newborn values from pediatric age groups |
| Ignoring age in hours/days | Early transition affects interpretation | Consider timing after birth |
| Not considering gestational age where relevant | Preterm and term newborns may differ | Follow maternal-newborn guidance |
| Forgetting temperature route | Route changes interpretation | Document axillary, rectal, temporal, or other route per policy |
| Exposing newborn too long during assessment | Heat loss can occur quickly | Minimize unnecessary exposure |
| Missing respiratory effort cues | RR alone may miss distress | Observe flaring, grunting, retractions, color, and tone |
| Trusting monitor readings without checking newborn appearance | Device artifact can occur | Check newborn, probe/cuff, waveform, and context |
| Not documenting crying, feeding, bathing, or skin-to-skin | Context explains changes | Add relevant newborn state/context |
| Ignoring trends | A changing pattern may matter | Compare with previous readings |
| Failing to report concerning changes | Delayed communication can affect safety | Report according to policy |
| Overfocusing on one number | Newborn assessment requires cue clustering | Assess temperature, HR, RR, color, tone, effort, feeding, and trend |
When to Report Newborn Vital Signs
Report newborn vital signs according to facility parameters, maternity/newborn unit policy, instructor or preceptor guidance, provider orders, early warning systems if used, and newborn condition.
Report when there are:
- Sudden changes from baseline
- Worsening trends
- Readings outside assigned parameters
- Readings inconsistent with newborn appearance
- Respiratory effort cues such as grunting, nasal flaring, or retractions
- Color change
- Poor tone or reduced responsiveness
- Feeding difficulty with concerning cues
- Temperature concerns
- SpO2 concerns if monitored
- Device readings that remain concerning after reassessment
- Any uncertainty about interpretation
Escalate uncertainty rather than guessing. Students should not diagnose newborn conditions or provide treatment instructions. The safer role is to reassess within scope, document accurately, and report using objective findings and relevant context.
How to Study Newborn Vital Signs for Nursing School
Start by learning adult vital signs, then separate newborn values clearly. Do not group newborns with older pediatric ranges.
Use these strategies:
- Memorize common newborn temperature, heart rate, and respiratory rate ranges.
- Learn why thermoregulation matters.
- Study respiratory transition after birth.
- Practice counting newborn respirations carefully.
- Practice documentation examples with route, time, state, and context.
- Use case scenarios to cluster cues.
- Review feeding, crying, sleep, bathing, and exposure as context.
- Learn how SpO2 can be affected by probe placement and movement.
- Ask instructors which ranges and documentation expectations your program uses.
- Practice explaining when to reassess and when to report.
Newborn vital signs become easier when students stop thinking only in numbers and start thinking in newborn-specific assessment patterns.
When to Ask for Help With Newborn Vital Signs Assignments
Students may need help with newborn assessment assignments, maternity/newborn case studies, documentation examples, care plans, clinical reflections, or vital signs interpretation questions. Academic support can help with organizing answers, explaining cue clustering, and applying newborn nursing assessment concepts to assignment instructions.
For coursework support, students can review nursing assignment help, nursing case study help, or healthcare assignment help. These links fit best here because this section focuses on assignments, documentation examples, case study reasoning, and academic guidance rather than clinical decision-making.
FAQs About Newborn Vital Signs
1. What are newborn vital signs?
Newborn vital signs are measurable assessment findings used to evaluate newborn physiological status. They commonly include temperature, heart rate, and respiratory rate. Oxygen saturation and blood pressure may be assessed depending on setting, screening, acuity, order, or facility policy.
2. What are normal newborn vital signs?
Commonly cited newborn ranges include heart rate 120–160 bpm, respiratory rate 40–60 breaths/min, systolic blood pressure 60–90 mmHg, and temperature 35.6°C–37.5°C in one newborn reference table (OpenStax/NCBI Bookshelf, n.d.). Ranges vary by source, gestational age, age in hours or days, clinical condition, and facility policy.
3. How are newborn vital signs different from pediatric vital signs?
Newborn vital signs focus on early transition after birth, thermoregulation, respiratory adaptation, feeding/activity effects, skin color, tone, and newborn-specific documentation. Older pediatric vital signs focus on age groups such as infant, toddler, preschool, school-age, and adolescent.
4. What is a normal newborn heart rate?
A commonly cited newborn heart rate is 120–160 bpm, but interpretation depends on sleep, crying, feeding, activity, temperature, gestational age where relevant, and clinical condition (Elshazzly et al., 2023).
5. What is a normal newborn respiratory rate?
A commonly cited newborn respiratory rate is 40–60 breaths per minute. Neonatal respirations should be counted carefully because breathing may be irregular, and effort cues such as grunting, nasal flaring, and retractions are important (MSD Manual Professional Edition, 2023).
6. Why is newborn temperature important?
Newborn temperature is important because newborns can lose heat easily and rely on immature thermoregulation mechanisms. Temperature should be interpreted with route, environment, exposure, feeding/activity, gestational age, and newborn condition.
7. Is newborn blood pressure always measured?
No. Newborn blood pressure may not be routine in all well-newborn settings. It may be assessed depending on acuity, provider order, clinical context, or facility policy.
8. How should newborn vital signs be documented?
Document value, unit, time, route or site, method if required, newborn state, oxygen context if applicable, relevant context such as crying or feeding, reassessment, and who was notified when required.
9. When should nursing students report newborn vital signs?
Students should report sudden changes, worsening trends, values outside assigned parameters, respiratory effort cues, color change, poor tone, feeding concerns with abnormal cues, readings inconsistent with newborn appearance, or any uncertainty according to facility policy and instructor or preceptor guidance.
10. What is the best way to study newborn vital signs?
Study newborn values separately from adult and older pediatric values. Focus on thermoregulation, respiratory transition, newborn-specific ranges, documentation, cue clustering, and the factors that affect readings, such as crying, feeding, bathing, sleep, and environmental exposure.
Final Thoughts on Newborn Vital Signs
Newborn vital signs require newborn-specific interpretation. Normal ranges are only a starting point. Thermoregulation, respiratory transition, age in hours or days, gestational age, feeding, crying, activity, skin color, tone, perfusion, trends, and measurement technique all matter.
Nursing students should learn accurate measurement, documentation, reassessment, cue clustering, and reporting. A single value should never be used to diagnose a newborn condition or dismiss concerning cues.
Newborn vital sign assessment must follow facility policy, instructor guidance, provider orders, newborn condition, scope of practice, and clinical judgment.
If students need help with newborn vital signs assignments, maternity/newborn nursing case studies, clinical reflection, documentation examples, or care plan interpretation, they can upload their instructions and rubric for academic guidance.
References
Elshazzly, M., Lopez, M. J., & Reddy, V. (2023). Physiology, newborn. StatPearls/NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK499951/
MedlinePlus. (2025). Changes in the newborn at birth. U.S. National Library of Medicine. https://medlineplus.gov/ency/article/002395.htm
MedlinePlus. (2025). Infant-newborn development. U.S. National Library of Medicine. https://medlineplus.gov/ency/article/002004.htm
MSD Manual Professional Edition. (2023). Physical examination of the newborn. https://www.msdmanuals.com/professional/pediatrics/care-of-newborns-and-infants/physical-examination-of-the-newborn
OpenStax/NCBI Bookshelf. (n.d.). Table 12.5c, normal newborn vital signs. National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK615345/table/ch12.tab4/
Sapra, A., Malik, A., & Bhandari, P. (2023). Vital sign assessment. StatPearls/NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK553213/
Torp, K. D., Modi, P., & Simon, L. V. (2023). Pulse oximetry. StatPearls/NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK470348/