Normal vital signs are essential for nursing assessment, but many students memorize ranges without knowing how to interpret them by age, baseline, symptoms, trends, activity, measurement method, and patient context.
This guide explains normal adult vital signs, pediatric and newborn overviews, older adult considerations, temperature, pulse, respiratory rate, blood pressure, oxygen saturation, baseline versus range, trends, documentation, cue clustering, and common student mistakes. This guide is for nursing education and clinical skills learning only. Vital sign assessment and response must follow facility policy, instructor guidance, provider orders, patient condition, scope of practice, and clinical judgment.
For students who need the full assessment overview, the complete vital signs guide covers the broader topic, including temperature, pulse, respiratory rate, blood pressure, oxygen saturation, pain assessment, measurement technique, documentation, trends, abnormal findings, and cue clustering. This article stays focused on normal vital signs and how students should interpret normal ranges safely.
Quick Answer: What Are Normal Vital Signs?
Normal vital signs are commonly cited reference ranges used to compare temperature, pulse, respiratory rate, blood pressure, and oxygen saturation.
Normal ranges vary by age, source, baseline, activity level, condition, medications, measurement method, and clinical setting.
Adult ranges are easier to memorize, but pediatric and newborn values require age-specific interpretation.
A value within a normal range does not always mean the patient is stable.
A value outside a normal range does not automatically confirm a diagnosis.
Nurses interpret vital signs with trends, symptoms, baseline, assessment findings, and facility guidance.
What Does “Normal Vital Signs” Mean in Nursing?
Normal vital signs are reference ranges, not absolute rules. They help nurses recognize whether a patient’s values are expected, changed from baseline, or potentially concerning. Traditional vital signs include temperature, pulse, respiratory rate, and blood pressure, while oxygen saturation is commonly assessed because it adds important cardiopulmonary context (Sapra et al., 2023).
In nursing, normal does not mean “ignore.” Normal means the value falls within a commonly cited range for many people in a similar age group. Students still need to ask: Is this normal for this patient? Is it different from baseline? Does it match the patient’s symptoms? Was the reading measured correctly?
Vital signs are objective data because they are measurable findings. However, objective data should be interpreted alongside subjective symptoms. A patient who reports dizziness, shortness of breath, severe pain, weakness, feeling faint, or “not feeling right” still needs attention even when the numbers look normal.
That is why nursing students should avoid two unsafe habits. The first is assuming a normal value proves the patient is stable. The second is assuming an abnormal value automatically confirms a diagnosis. Both mistakes ignore the full nursing assessment.
Normal Vital Signs Chart by Age
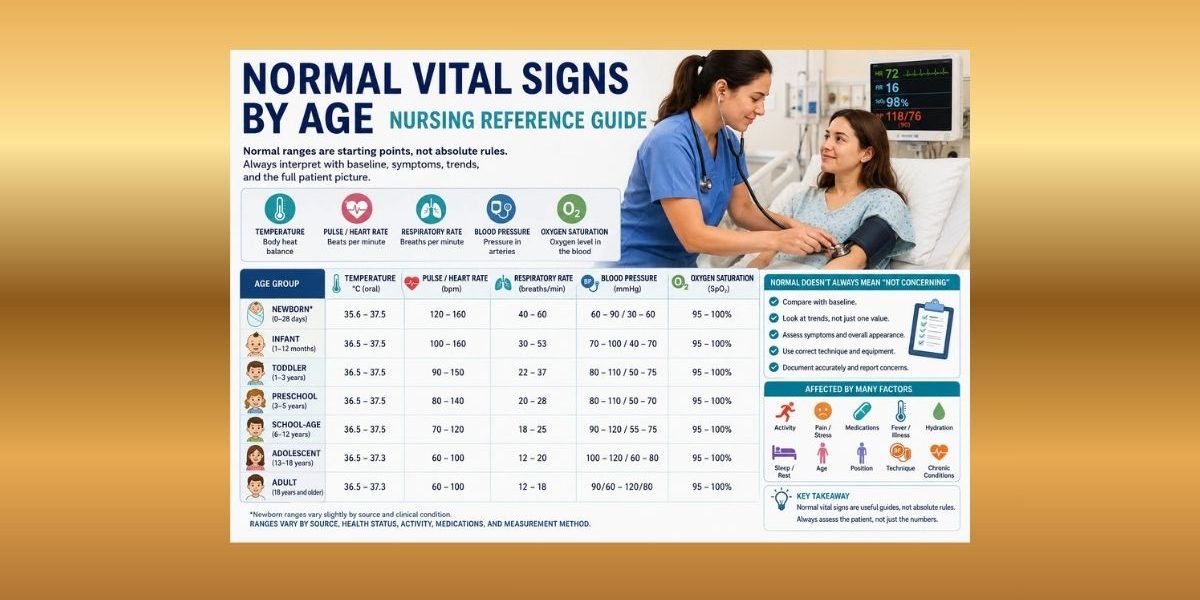
The chart below gives a practical nursing reference for normal vital signs by age. Use it as a learning guide, not a diagnostic rule. Ranges vary by source, institution, patient baseline, condition, measurement method, and clinical context. Pediatric ranges especially vary across references, and patterns of change can be as important as the listed thresholds (Royal Children’s Hospital Melbourne, 2023).
| Age group | Temperature | Pulse/heart rate | Respiratory rate | Blood pressure overview | Oxygen saturation overview | Nursing notes |
|---|---|---|---|---|---|---|
| Adult | Commonly cited oral range about 36.5°C–37.3°C | Commonly cited range 60–100 bpm | Commonly cited range 12–18/min | Often cited around 90/60 to 120/80 mmHg | Often expected in the mid-to-high 90s on room air in many healthy adults | Interpret with baseline, symptoms, activity, pain, medications, and measurement technique |
| Older adult considerations | Similar reference ranges may be used, but baseline matters | May be affected by medications, fitness, pain, infection, hydration, or conduction issues | May change subtly with illness, pain, anxiety, or respiratory disease | Chronic conditions and medications may affect BP | Interpret with respiratory effort, color, mentation, perfusion, and device accuracy | Do not assume abnormal findings are “normal for age” |
| Adolescent overview | Similar to adult by later adolescence | Often approaches adult range | Often approaches adult range | BP interpretation depends on age and guideline context | Interpret with symptoms, activity, and device quality | Privacy, anxiety, caffeine, pain, hydration, and medications may affect readings |
| School-age child overview | Depends on route and condition | Commonly higher than adults in younger school-age children | Often faster than adults | BP varies with age, size, and height | Interpret with respiratory effort and appearance | Use age-based pediatric context |
| Preschool child overview | Depends on route and condition | Often faster than adults | Often faster than adults | Correct cuff size is essential | Motion can affect readings | Fear, crying, and activity can change values |
| Toddler overview | Depends on route and condition | Often faster than adults | Often faster than adults | BP may be affected by movement and distress | Probe placement and motion matter | Document crying, activity, or distress when relevant |
| Infant overview, excluding immediate newborn context | Depends on route and condition | Higher than adult values | Higher than adult values | Lower than older children and adults | Interpret with color, feeding, respiratory effort, and probe quality | Do not use adult ranges |
| Newborn overview | Approximate newborn ranges differ from older children | Common newborn HR range often 120–160 bpm | Common newborn RR range often 40–60/min | Newborn BP differs from older children | Interpret with transition, color, feeding, breathing, and policy | Newborn vital signs deserve separate focused study |
MedlinePlus lists adult reference values such as blood pressure between 90/60 and 120/80 mmHg, breathing 12–18 breaths per minute, pulse 60–100 beats per minute, and temperature 36.5°C–37.3°C, while also noting that normal values vary with age, weight, health, and exercise capacity (MedlinePlus, 2025).
A future vital signs chart article can provide a more printable quick-reference format. This guide focuses on interpretation, context, documentation, and safe nursing thinking.
Normal Adult Vital Signs
Normal adult vital signs are often the first ranges students memorize. Common adult references usually include temperature around 36.5°C–37.3°C, pulse 60–100 bpm, respiratory rate 12–18/min, and blood pressure around 90/60 to 120/80 mmHg (MedlinePlus, 2025).
These values are useful, but they are not enough. Activity, anxiety, pain, medications, hydration, illness, caffeine, nicotine, body position, time of day, and measurement technique can affect readings.
For example, an adult pulse of 98 bpm may technically fall within a commonly cited range, but it may still matter if that patient’s usual resting pulse is 62 bpm and the patient now feels weak or short of breath. A respiratory rate of 18/min may appear normal, but shallow breathing, accessory muscle use, or new confusion would add concern.
Normal adult vital signs should always be interpreted with baseline and symptoms. Students should learn the numbers, but they should also learn what the numbers mean in the patient’s full clinical picture.
Normal Vital Signs for Older Adults
Older adults should not be treated as if abnormal vital signs are automatically normal because of age. At the same time, students should not assume every older adult has the same baseline.
Medications, chronic conditions, hydration status, mobility, pain, infection, frailty, autonomic changes, and cardiac or respiratory history may affect vital signs. Some older adults may show subtle changes rather than dramatic changes. For example, a small rise in respiratory rate, mild confusion, new weakness, or a change from baseline may be more meaningful than a single number alone.
The safest nursing habit is to compare current vital signs with the patient’s usual baseline when available. Ask whether the patient looks different, reports new symptoms, has changed activity tolerance, or has a trend that is moving in the wrong direction.
Do not normalize concerning findings by saying, “That is just because the patient is old.” Instead, reassess, document, and report according to facility policy, instructor guidance, and patient condition.
Normal Pediatric Vital Signs Overview
Normal pediatric vital signs vary by age. Younger children often have faster pulse and respiratory rates than adults. Pediatric blood pressure also changes with age, size, height, sex, and technique.
Pediatric assessment requires context. Crying, fever, activity, fear, pain, sleep, feeding, cuff size, probe placement, and cooperation can affect readings. The Royal Children’s Hospital provides age-based ranges for systolic blood pressure, heart rate, and respiratory rate and emphasizes that changes over time matter, not just isolated thresholds (Royal Children’s Hospital Melbourne, 2023).
This section is only an overview. A dedicated pediatric vital signs article can go deeper into infant, toddler, preschool, school-age, and adolescent ranges, plus pediatric-specific documentation and cue clustering.
Normal Newborn Vital Signs Overview
Newborn vital signs differ from older children and adults. Newborn assessment includes unique concerns related to thermoregulation, respiratory transition, feeding, color, tone, and adaptation after birth.
One NCBI nursing table lists normal newborn values including heart rate 120–160 bpm, respiratory rate 40–60 breaths per minute, systolic blood pressure 60–90 mmHg, and temperature around 35.6°C–37.5°C, depending on context and source (OpenStax/NCBI Bookshelf, n.d.).
Newborn vital signs should not be merged casually with general pediatric vital signs. A newborn can have expected values that look abnormal beside adult ranges. Students should study newborns separately and follow maternal-newborn or pediatric clinical guidance.
Normal Temperature Range
Normal temperature depends on route, measurement method, age, activity, time of day, environment, recent intake, recent bathing, medications, and illness. Oral, tympanic, temporal, axillary, and rectal routes may produce different readings.
Johns Hopkins Medicine notes that adult body temperature can vary with recent activity, food and fluid intake, time of day, and measurement route. It also explains that rectal temperatures tend to be higher than oral readings, while axillary temperatures tend to be lower (Johns Hopkins Medicine, 2025).
Students must document the route. “Temperature 37.8°C” is less complete than “Temperature 37.8°C tympanic.” Route matters because a value may be interpreted differently depending on how it was obtained.
Do not use a temperature value alone to diagnose infection, fever cause, hypothermia cause, or treatment need. Document the reading, route, time, symptoms, and relevant context. Report according to facility policy and instructor or preceptor guidance.
Normal Pulse Rate and Heart Rate
Pulse rate reflects the number of heartbeats per minute felt at a pulse site. Heart rate may also be measured apically or by a monitor, depending on the setting and skill.
For many adults, 60–100 bpm is a commonly cited resting pulse range (MedlinePlus, 2025). However, pulse varies with age, activity, fever, pain, anxiety, hydration, medications, fitness level, illness, and emotional stress.
Pulse quality, rhythm, and strength may matter. A pulse may be regular or irregular, strong or weak, equal or unequal, depending on what the assessment requires. Students should follow the expected clinical skill and documentation standard.
A pulse within range should still be compared with baseline. A patient whose pulse rises from 58 to 96 bpm may still be within a common adult range, but that change could be meaningful if paired with dizziness, pain, fever, shortness of breath, bleeding concern, dehydration cues, or new weakness.
Documentation examples:
“HR 82 bpm, radial, regular.”
“Apical pulse 96 bpm, regular, patient reports pain 7/10.”
“Pulse 104 bpm after ambulation; reassessed after rest per instructor guidance.”
Normal Respiratory Rate
Respiratory rate is the number of breaths per minute. For adults, 12–18 breaths per minute is a commonly cited reference range in MedlinePlus (2025). Pediatric respiratory rates are usually faster, especially in infants and younger children.
Respirations are often undercounted by students because the patient is talking, moving, or being observed too briefly. Respiratory rate should be counted carefully according to skills-lab and facility guidance.
Respiratory effort matters as much as the number. A patient may have a normal respiratory rate but still show shallow breathing, accessory muscle use, pursed-lip breathing, inability to speak comfortably, abnormal breath sounds, fatigue, or anxiety. In children, nasal flaring, retractions, grunting, posture, poor feeding, or decreased play may add concern.
Documentation examples:
“RR 18/min, unlabored, room air.”
“RR 20/min, shallow respirations noted.”
“RR 24/min after activity; patient reports shortness of breath; nurse notified according to policy.”
Normal Blood Pressure
Blood pressure measures the force of blood against artery walls during heart contraction and relaxation. Adult blood pressure is often taught using commonly cited categories, but students should avoid oversimplifying BP into one universal normal value.
MedlinePlus lists adult blood pressure between 90/60 and 120/80 mmHg as a commonly cited normal range (MedlinePlus, 2025). However, interpretation depends on patient baseline, symptoms, position, activity, pain, anxiety, medications, hydration, and clinical context.
Pediatric blood pressure is more complex. In children, BP interpretation can depend on age, sex, height, and measurement technique. The MSD Manual Professional Edition explains that correct cuff size is critical and that cuff width should be at least 40% of mid-upper-arm circumference, with bladder length covering 80% to 100% of the arm circumference (MSD Manual Professional Edition, 2025).
Technique affects BP. A cuff that is too small may give a falsely high reading. A cuff that is too large may give a falsely low reading. Arm position, body position, movement, talking, crossed legs, unsupported back, anxiety, and recent activity can also affect readings.
Automated readings are useful, but unexpected readings may need manual verification according to policy. Students should not copy a questionable value without checking the patient, cuff, position, and device.
Normal Oxygen Saturation
Oxygen saturation, often documented as SpO2, estimates the percentage of hemoglobin saturated with oxygen. Pulse oximetry can help clarify cardiopulmonary status when traditional vital signs do not tell the full story (Sapra et al., 2023).
Normal oxygen saturation is commonly expected in the mid-to-high 90s for many healthy patients on room air, but students should avoid using one universal number without context. Oxygen therapy, chronic respiratory disease, acute illness, perfusion, probe placement, nail products, cold extremities, movement, skin pigmentation considerations, and device error may affect interpretation or accuracy.
SpO2 should be interpreted with respiratory effort, mental status, skin color, symptoms, oxygen device if present, work of breathing, and trend. A normal SpO2 does not always mean breathing is normal. A patient may maintain oxygen saturation while working harder to breathe.
Do not use this section as oxygen administration guidance. Oxygen therapy and device changes must follow provider orders, facility policy, scope of practice, and instructor or preceptor direction.
Baseline Vital Signs vs Normal Ranges
Baseline vital signs are the patient’s usual values. Normal ranges are commonly cited reference values. Nursing students need both.
A value may be within a normal range but abnormal for that patient if it changes sharply from baseline. A value may fall outside a generic range but be expected for a known patient context only when supported by assessment findings, history, and clinical guidance.
| Situation | Why range alone is not enough | Nursing thinking |
|---|---|---|
| HR 96 bpm in an adult whose usual HR is 58 bpm | The value is within a common adult range but sharply changed | Compare with symptoms, pain, fever, activity, medications, and trend |
| BP 100/64 mmHg in a patient who reports dizziness | The number may look acceptable, but symptoms matter | Assess position, trend, baseline, and report according to policy |
| SpO2 96% with visible work of breathing | Saturation may look normal while breathing effort is abnormal | Assess respiratory effort, pattern, color, symptoms, and report concerns |
| RR 18/min with severe pain | Respiratory rate alone does not measure pain severity | Assess pain using an appropriate tool and document response |
| Temperature 37.2°C in a patient with new confusion | Temperature alone does not rule out illness | Cluster cues and report change in condition according to guidance |
Students should avoid assuming “normal” means “not important.” A normal value is one piece of assessment data, not the whole assessment.
Vital Sign Trends vs One-Time Normal Readings
One reading can be misleading. The patient may have just walked, cried, coughed, moved, taken medication, experienced pain, or been measured with incorrect technique. Trends show direction of change.
Trend interpretation asks:
- Is the value rising, falling, or staying stable?
- Is the change expected after activity, rest, pain, or a procedure?
- Does the value match the patient’s condition?
- Is the patient reporting symptoms?
- Does the trend differ from baseline?
- Was the measurement technique reliable?
A patient with normal vital signs at 0800 may still need reassessment if values trend upward by 1000 and the patient reports dizziness or shortness of breath. A child with a respiratory rate near the upper range may need closer attention if the rate keeps rising and work of breathing increases.
Students should repeat abnormal or unexpected readings according to facility policy. They should document reassessment and report concerning trends according to instructor, preceptor, nurse, provider, or facility guidance.
Factors That Can Change Normal Vital Signs
| Factor | Vital signs affected | Nursing consideration |
|---|---|---|
| Age | HR, RR, BP, temperature interpretation | Use age-appropriate ranges |
| Activity | HR, RR, BP, temperature | Allow rest when required before measurement |
| Pain | HR, RR, BP, behavior | Assess pain separately using an appropriate tool |
| Anxiety/stress | HR, RR, BP | Reassure, explain, and reassess when appropriate |
| Fever/infection | Temperature, HR, RR | Cluster with symptoms and patient condition |
| Medications | HR, BP, RR, temperature | Consider prescribed effects within student scope |
| Hydration/fluid status | HR, BP, perfusion cues | Compare with intake, output, mucous membranes, and symptoms |
| Posture | BP, RR, SpO2 | Document position when relevant |
| Oxygen therapy | SpO2, RR, work of breathing | Document device and flow if required |
| Chronic conditions | All vital signs | Compare with baseline and care plan |
| Environment | Temperature, HR, RR | Consider room temperature, clothing, and exposure |
| Measurement technique | All vital signs | Check route, cuff size, site, timing, and device placement |
| Recent procedures | HR, RR, BP, pain | Consider pain, anxiety, sedation, and recovery context |
| Sleep/rest | HR, RR, BP | Sleeping values may differ from awake values |
| Caffeine/nicotine where relevant | HR, BP | Consider recent intake when clinically relevant |
When a Normal Vital Sign May Still Be Concerning
A within-range vital sign may still need attention when it does not match the patient’s condition. This is one of the biggest clinical judgment lessons for nursing students.
A “normal” blood pressure may still matter if the patient feels dizzy when standing. A normal oxygen saturation may not be reassuring if the patient has increased work of breathing. A pulse may fall within a normal adult range but still represent a sharp increase from baseline. Severe pain can exist even when vital signs are normal.
Examples:
Normal blood pressure with dizziness on standing: A patient has BP 112/70 mmHg but reports dizziness when getting up. The number looks acceptable, but the symptom matters. The student should reassess according to policy and report the concern.
Normal oxygen saturation but increased work of breathing: A patient has SpO2 96% on room air but uses accessory muscles and speaks in short phrases. The saturation alone does not erase the respiratory cues.
Normal pulse range but sharp increase from baseline: A patient’s HR rises from 62 to 96 bpm. The value is within a common adult range, but the change may matter if paired with symptoms or a worsening trend.
Normal vital signs with severe reported pain: A patient reports pain 9/10. Normal pulse and blood pressure do not prove the pain is mild or absent.
Students should report according to facility policy and instructor or preceptor guidance. Do not diagnose or recommend treatment from these examples.
How to Measure Normal Vital Signs Accurately
Accurate vital signs require correct technique. A normal value measured poorly may be falsely reassuring.
Use this practical checklist:
- Prepare the patient and explain what you are doing.
- Confirm identity according to facility policy.
- Use correct equipment.
- Choose the correct blood pressure cuff size.
- Position the patient appropriately.
- Document the temperature route.
- Count respirations accurately.
- Check oxygen saturation probe placement and signal quality.
- Verify unusual readings.
- Compare values with baseline and symptoms.
- Repeat the reading when it does not match patient condition.
- Follow facility policy and instructor guidance.
This checklist does not replace skills-lab training or clinical procedure manuals. It supports safe thinking while students practice normal vital signs nursing assessment.
Normal Vital Signs Documentation in Nursing
Vital signs documentation should be accurate, clear, and complete. Nursing documentation should include the value, unit, time, route or site, position when relevant, oxygen device if applicable, pain score if required, and relevant context.
Open RN documentation guidance describes vital signs as including temperature, pulse, respiratory rate, blood pressure, and oxygen saturation, and notes that pain ratings are often considered alongside vital signs (Reuter-Sandquist, 2022).
Examples of clear documentation:
“Temperature 36.9°C oral at 0800.”
“HR 82 bpm, radial, regular.”
“RR 18/min, unlabored, room air.”
“BP 118/72 mmHg, right arm, sitting.”
“SpO2 97% on room air.”
“Pain 6/10; patient guarding abdomen; nurse notified per policy.”
Avoid vague documentation such as “vitals normal” when the actual values, route, and context should be charted. Use facility-approved abbreviations only.
Common Mistakes Students Make With Normal Vital Signs
| Mistake | Why it matters | Safer habit |
|---|---|---|
| Memorizing numbers without context | Ranges do not explain the whole patient picture | Connect values with baseline, symptoms, and trends |
| Thinking normal means stable | A patient can be unwell with normal readings | Assess the patient, not only the chart |
| Ignoring baseline | A “normal” value may be abnormal for that patient | Compare current values with usual values |
| Missing trends | Direction of change can reveal worsening status | Review previous readings |
| Using adult ranges for children | Pediatric values differ by age | Use age-specific ranges |
| Merging newborn and pediatric values | Newborn transition is unique | Study newborns separately |
| Forgetting temperature route | Route affects interpretation | Document oral, tympanic, temporal, axillary, or rectal route |
| Using wrong cuff size | BP can be falsely high or low | Match cuff size to arm size |
| Trusting devices without checking patient condition | Devices can show artifact | Check patient, placement, and signal |
| Undercounting respirations | RR is easy to underestimate | Count carefully according to skill standards |
| Ignoring subjective symptoms | Symptoms add meaning to objective data | Cluster objective and subjective cues |
| Documenting without context | The chart may not explain the reading | Add activity, position, oxygen device, pain, or reassessment when relevant |
Normal Vital Signs and Cue Clustering Examples
Example 1: Normal SpO2 but Increased Work of Breathing
Scenario: A patient has SpO2 96% on room air.
Objective vital sign cues: Oxygen saturation appears within a commonly expected range.
Subjective patient cues: The patient says, “I feel short of breath.”
Other assessment cues: The patient uses accessory muscles and pauses while speaking.
Why the “normal” value may or may not be reassuring: The oxygen saturation alone does not explain breathing effort. Work of breathing and symptoms matter.
Appropriate student action: Reassess respiratory rate and effort, document findings, and report to the nurse, instructor, or preceptor according to policy.
Example 2: Normal BP but Dizziness on Standing
Scenario: A patient’s BP is 112/70 mmHg while sitting.
Objective vital sign cues: The BP appears within a commonly cited adult range.
Subjective patient cues: The patient reports dizziness when standing.
Other assessment cues: The patient looks unsteady and grips the bedrail.
Why the “normal” value may or may not be reassuring: A single seated BP does not explain positional symptoms.
Appropriate student action: Follow facility guidance for reassessment, maintain safety, document symptoms, and report the concern.
Example 3: Pulse Within Range but Trending Upward
Scenario: A patient’s pulse changes from 68 to 82 to 98 bpm over several checks.
Objective vital sign cues: The final value may still fall within a common adult range.
Subjective patient cues: The patient reports feeling weak and “not right.”
Other assessment cues: The patient appears pale and less interactive.
Why the “normal” value may or may not be reassuring: The trend matters more than the isolated number.
Appropriate student action: Reassess, compare with other vital signs, document the trend, and report according to clinical guidance.
Example 4: Normal Vital Signs With Severe Pain
Scenario: A postoperative patient has HR 88 bpm, BP 122/76 mmHg, RR 18/min, and SpO2 98% on room air.
Objective vital sign cues: The vital signs look within common adult ranges.
Subjective patient cues: The patient reports pain 9/10.
Other assessment cues: The patient grimaces and avoids movement.
Why the “normal” value may or may not be reassuring: Normal vital signs do not prove pain is absent or mild.
Appropriate student action: Document pain using the required scale or tool, report according to policy, and reassess as directed.
When to Report Vital Signs That Are “Normal”
Students should report vital signs that are “normal” when the full patient picture is not reassuring. Reporting depends on facility parameters, instructor or preceptor guidance, provider orders, early warning systems if used, and patient condition.
Report when there are:
- Concerning symptoms
- Sharp changes from baseline
- Worsening trends
- Values inconsistent with appearance
- Readings that do not match patient condition
- New dizziness, weakness, shortness of breath, confusion, severe pain, or distress
- Questionable device readings that remain concerning after reassessment
- Uncertainty about interpretation
Escalate uncertainty rather than guessing. Students do not need to diagnose the problem before asking for help. They should communicate clearly: what was measured, what changed, what the patient reports, what was observed, and what reassessment was done.
How to Study Normal Vital Signs for Nursing School
Learn adult ranges first because they form the foundation. Then study pediatric and newborn ranges separately. Do not rely on memorization alone.
Use these study strategies:
- Create a simple adult vital signs range card.
- Study pediatric age groups separately.
- Keep newborn values separate from older pediatric values.
- Practice connecting numbers to patient scenarios.
- Learn factors that change readings.
- Practice documentation examples.
- Compare baseline versus current readings.
- Review common technique errors.
- Ask instructors which ranges your program expects.
- Use case studies to practice cue clustering.
The strongest students know both the ranges and the reasoning behind the ranges.
When to Ask for Help With Normal Vital Signs Assignments
Students may need help with nursing assessment assignments, case studies, documentation examples, care plans, clinical reflections, or vital-sign interpretation questions. Academic support can help with organizing answers, explaining cue clustering, and applying nursing assessment concepts to assignment instructions.
For assignment-focused support, students can review nursing assignment help, nursing case study help, or healthcare assignment help.
FAQs About Normal Vital Signs
1. What are normal vital signs?
Normal vital signs are commonly cited reference ranges for temperature, pulse, respiratory rate, blood pressure, and oxygen saturation. They help nurses compare a patient’s values with expected ranges while still considering baseline, symptoms, trends, and context.
2. What are normal adult vital signs?
Common adult references include temperature around 36.5°C–37.3°C, pulse 60–100 bpm, respiratory rate 12–18/min, and blood pressure around 90/60 to 120/80 mmHg (MedlinePlus, 2025).
3. What are normal vital signs by age?
Normal vital signs by age differ across newborns, infants, children, adolescents, adults, and older adults. Younger children often have faster pulse and respiratory rates than adults. Newborn values differ from older pediatric values.
4. Are pediatric vital signs different from adult vital signs?
Yes. Pediatric vital signs vary by age, size, developmental stage, activity, crying, fever, fear, and measurement technique. Adult ranges should not be applied to children.
5. Are newborn vital signs different from pediatric vital signs?
Yes. Newborn vital signs have unique transition and thermoregulation considerations. Newborns should be studied separately from older infants and children.
6. What is a normal blood pressure?
For many adults, 90/60 to 120/80 mmHg is a commonly cited normal range (MedlinePlus, 2025). However, blood pressure interpretation depends on baseline, symptoms, age, position, activity, cuff size, medications, and clinical condition.
7. What is a normal respiratory rate?
A commonly cited adult respiratory rate is 12–18 breaths per minute (MedlinePlus, 2025). Children and newborns usually have faster respiratory rates, so age-specific interpretation is required.
8. What is a normal oxygen saturation?
Many healthy patients on room air are expected to have oxygen saturation in the mid-to-high 90s, but interpretation depends on respiratory effort, symptoms, oxygen use, perfusion, device accuracy, and baseline.
9. Can vital signs be normal when a patient is still unwell?
Yes. A patient may have normal-looking vital signs but still report severe pain, dizziness, shortness of breath, weakness, or other concerning symptoms. Nurses interpret vital signs with the full assessment.
10. How should normal vital signs be documented?
Document the value, unit, time, route or site, position if relevant, oxygen device if applicable, pain score if required, and important context. Examples include “Temperature 36.9°C oral at 0800” and “BP 118/72 mmHg, right arm, sitting.”
Final Thoughts on Normal Vital Signs
Normal vital signs are reference ranges, not absolute proof of stability. Age, baseline, trends, symptoms, activity, technique, medications, pain, oxygen use, and patient condition all matter.
Nursing students should learn the ranges, but they should also learn how to interpret them in context. A normal value can still require reassessment when it does not match the patient’s symptoms, baseline, or appearance. An abnormal value should be reassessed and reported according to policy rather than used alone to diagnose a condition.
Vital sign assessment must follow facility policy, instructor guidance, scope of practice, provider orders, patient condition, and clinical judgment.
If students need help with normal vital signs assignments, nursing assessment case studies, clinical reflection, documentation examples, or care plan interpretation, they can upload their instructions and rubric for academic guidance.
References
Johns Hopkins Medicine. (2025). Vital signs (body temperature, pulse rate, respiration rate, blood pressure). https://www.hopkinsmedicine.org/health/conditions-and-diseases/vital-signs-body-temperature-pulse-rate-respiration-rate-blood-pressure
MedlinePlus. (2025). Vital signs. U.S. National Library of Medicine. https://medlineplus.gov/ency/article/002341.htm
MSD Manual Professional Edition. (2025). Hypertension in children. https://www.msdmanuals.com/professional/pediatrics/hypertension-in-children/hypertension-in-children
OpenStax/NCBI Bookshelf. (n.d.). Table 12.5c, normal newborn vital signs. National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK615345/table/ch12.tab4/
Reuter-Sandquist, M. (2022). Nursing assistant: Chapter 7, demonstrate reporting and documentation. Open RN/NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK599391/
Royal Children’s Hospital Melbourne. (2023). Clinical practice guidelines: Acceptable ranges for physiological variables. https://www.rch.org.au/clinicalguide/guideline_index/normal_ranges_for_physiological_variables/
Sapra, A., Malik, A., & Bhandari, P. (2023). Vital sign assessment. StatPearls/NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK553213/