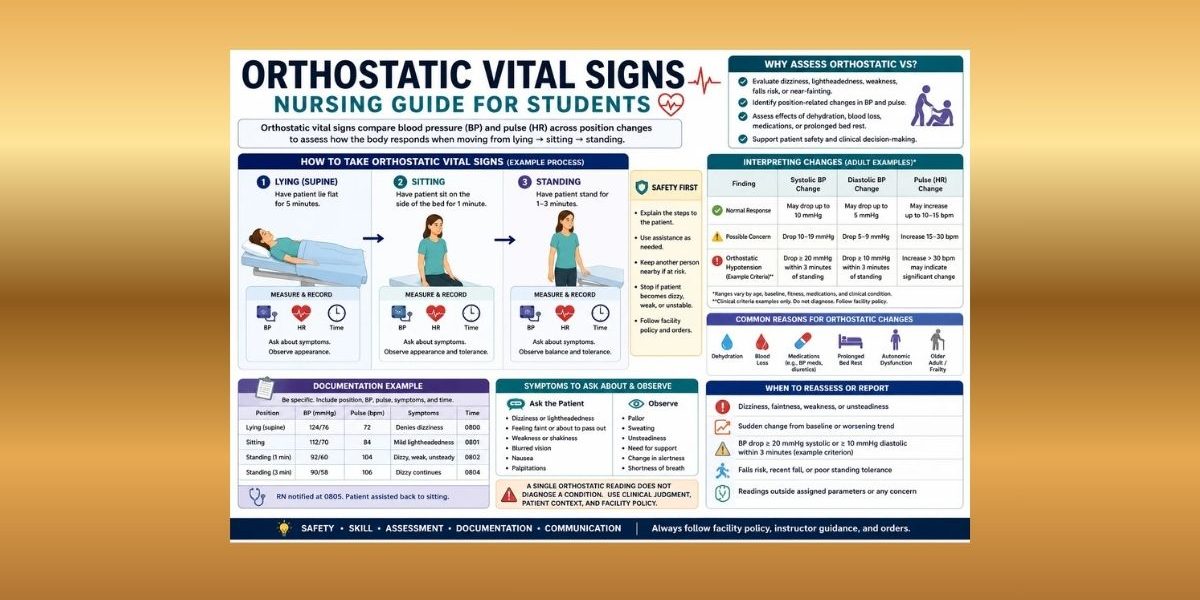
Orthostatic vital signs help nursing students compare blood pressure and pulse across position changes, usually lying, sitting, and standing, while watching for symptoms.
Many nursing students understand routine vital signs but become unsure when readings must be compared across positions. Orthostatic assessment requires more than recording numbers. Students must observe dizziness, lightheadedness, weakness, blood pressure changes, pulse changes, patient safety, timing, technique, and falls risk.
This article explains what orthostatic vital signs are, why they are assessed, how lying/sitting/standing readings are compared, how blood pressure and pulse changes are interpreted in context, how symptoms are documented, and when findings require reassessment or reporting. This guide is for nursing education and clinical skills learning only. Orthostatic vital sign assessment and response must follow facility policy, instructor guidance, provider orders, patient condition, scope of practice, and clinical judgment.
For students who need the broader foundation first, the complete vital signs guide covers temperature, pulse, respiratory rate, blood pressure, oxygen saturation, pain assessment, measurement technique, documentation, trends, abnormal findings, and cue clustering. This supporting article stays focused on orthostatic vital signs and position-change assessment.
Quick Answer: What Are Orthostatic Vital Signs?
- Orthostatic vital signs are vital sign measurements taken across position changes, commonly lying, sitting, and standing according to policy.
- They usually focus on blood pressure and pulse changes.
- They are often assessed when symptoms such as dizziness, lightheadedness, weakness, falls risk, dehydration concerns, blood loss concerns, or medication effects are relevant.
- Readings should be interpreted with symptoms, baseline, patient condition, measurement technique, and facility policy.
- A single orthostatic reading does not diagnose a condition by itself.
- Nursing students should document position, readings, symptoms, timing, and who was notified when required.
What Are Orthostatic Vital Signs?
Orthostatic vital signs are blood pressure and pulse measurements collected during position changes. Depending on facility policy, readings may be taken while the patient is lying, sitting, and standing. Some protocols use lying and standing readings only. The key idea is comparison across positions, not just one blood pressure or pulse value.
Routine vital signs show the patient’s current physiological status. Orthostatic vital signs show how the patient’s blood pressure and pulse respond when the body changes position. This matters because standing shifts blood volume and requires the cardiovascular system to adjust. If adjustment is delayed, reduced, or poorly tolerated, the patient may report dizziness, lightheadedness, weakness, faintness, blurred vision, or unsteadiness.
Blood pressure and pulse are usually central because they show how circulation responds during position change. However, symptoms matter as much as the numbers. A patient who feels faint during standing should not be ignored because the reading looks “close enough.” A patient with a large blood pressure or pulse change also needs context, technique review, reassessment, and reporting according to clinical guidance.
Orthostatic assessment combines objective data and subjective symptoms. Objective data include blood pressure and pulse readings by position. Subjective symptoms include dizziness, lightheadedness, weakness, nausea, or feeling faint. Observable signs, such as pallor, diaphoresis, unsteadiness, or near-fall behavior, add more clinical context.
Why Orthostatic Vital Signs Matter in Nursing
Orthostatic vital signs may help identify concerning position-related changes in blood pressure and pulse. They can provide assessment data when a patient reports dizziness on standing, has a recent fall, appears weak, has possible dehydration concerns, has blood loss risk, is taking medications that may affect blood pressure, or has autonomic regulation concerns. These are assessment contexts, not automatic diagnoses.
Orthostatic assessment also supports patient safety. The patient may become dizzy or unsteady while sitting or standing. Nursing students should prepare for safe positioning, follow facility policy, and ask for help when unsure. The Centers for Disease Control and Prevention includes orthostatic blood pressure measurement within older adult fall-risk assessment resources, reflecting its relevance to fall prevention screening and clinical risk recognition (Centers for Disease Control and Prevention [CDC], 2024).
The readings also improve communication. Instead of saying, “The patient got dizzy,” a student can report, “Supine BP was / with HR ___; standing BP was / with HR ___; patient reported lightheadedness and appeared unsteady.” That gives the nurse, preceptor, or provider clearer objective and subjective data.
Orthostatic Vital Signs vs Routine Vital Signs
| Assessment type | What it measures | Typical focus | Nursing note |
|---|---|---|---|
| Routine vital signs | Current physiological status at one time or position | Temperature, pulse, respirations, BP, SpO2, pain where required | Useful for general assessment, trending, and baseline comparison |
| Orthostatic vital signs | Changes in BP and pulse across position changes | Lying/sitting/standing BP and pulse, plus symptoms | Useful when position-related symptoms, falls risk, hydration concerns, medication effects, or provider orders are relevant |
Routine vital signs answer: “What are the patient’s current readings?”
Orthostatic vital signs answer: “What happens to blood pressure, pulse, and symptoms when the patient changes position?”
That distinction matters. A routine sitting BP may appear acceptable, but the patient may become dizzy when standing. Orthostatic vital signs help organize that position-related assessment safely and clearly.
When Orthostatic Vital Signs May Be Assessed
Orthostatic vital signs may be assessed when the patient’s condition, symptoms, provider orders, facility protocol, or instructor guidance calls for position-change assessment.
Common assessment contexts include:
- Dizziness on standing
- Lightheadedness on standing
- Faintness or near-fainting
- Weakness with position changes
- Recent falls or falls risk
- Dehydration concerns
- Possible blood loss context
- Medication effects that may influence BP or pulse
- Prolonged bed rest
- Older adult assessment contexts
- Post-procedure monitoring when policy requires it
- Provider order or facility protocol
These contexts do not mean the student should diagnose the patient. They mean orthostatic readings may add useful assessment data. Merck Manual explains that orthostatic hypotension can be more pronounced in contexts such as dehydration, warmth, certain illnesses, and prolonged lying or sitting, and it may cause lightheadedness or fainting in some people (Merck Manual Consumer Version, 2024).
Lying, Sitting, and Standing Orthostatic Vital Signs
Orthostatic readings may be collected in lying, sitting, and standing positions depending on facility policy. Some facilities use lying and standing only. Others include sitting because symptoms may appear before the patient reaches full standing.
Timing also depends on policy. The CDC STEADI orthostatic blood pressure tool instructs clinicians to have the patient lie down for five minutes, measure blood pressure and pulse, have the patient stand, and repeat blood pressure and pulse measurements after standing according to its steps (CDC, 2024). MSD Manual Professional Edition describes measuring BP and heart rate after five minutes supine and at one and three minutes after standing, with seated assessment as an option when the patient cannot stand (MSD Manual Professional Edition, 2024).
Students should not rush or improvise beyond policy. Patient safety matters during every position change.
| Position | What students observe | What to document |
|---|---|---|
| Lying/supine | Baseline BP and pulse, symptoms at rest, comfort, skin signs, mental status | Position, BP, pulse, time, symptoms or absence of symptoms |
| Sitting | Dizziness, lightheadedness, pallor, weakness, balance, tolerance | Position, BP, pulse if required, symptoms, patient tolerance |
| Standing | BP and pulse response, dizziness, unsteadiness, faintness, weakness, safety risk | Position, BP, pulse, timing, symptoms, assistance needed, notification if required |
If symptoms occur, follow facility policy. Do not continue a position change assessment in an unsafe way just to complete a table.
Blood Pressure Changes With Position
Blood pressure may change when a patient moves from lying to sitting or standing. Orthostatic blood pressure assessment compares systolic and diastolic readings across positions. A decrease in blood pressure after standing may be clinically relevant, especially when paired with dizziness, lightheadedness, weakness, or falls risk.
Some references define orthostatic hypotension as a decrease of at least 20 mmHg systolic or 10 mmHg diastolic within three minutes of standing or head-up tilt, but nursing students should treat these as clinical reference criteria, not as independent permission to diagnose from one reading (Ringer et al., 2025). Facility parameters, provider orders, instructor guidance, patient baseline, symptoms, and measurement conditions still matter.
Technique can affect BP readings. Cuff size, arm position, body position, movement, talking, timing between positions, device accuracy, and anxiety may distort results. If a reading does not match the patient’s condition, reassess according to policy and ask for guidance.
Pulse Changes With Position
Pulse may increase when a patient stands. That increase can be a normal response in some situations, but a larger-than-expected or symptomatic pulse change may provide important context. Pulse changes should be interpreted with blood pressure, symptoms, hydration status, medications, activity level, anxiety, pain, and clinical condition.
MSD Manual Professional Edition notes that BP and heart rate are measured together during orthostatic assessment and that heart rate response can add useful context when interpreting positional changes (MSD Manual Professional Edition, 2024). Open RN nursing skills content also notes that pulse rate may be collected when obtaining orthostatic vital signs and that a significant pulse increase while standing or sitting, if unable to stand, can indicate a meaningful change (Ernstmeyer & Christman, 2023).
Students should avoid overinterpreting pulse alone. A patient may have an increased pulse because of pain, anxiety, recent activity, fever, dehydration concerns, medications, or other clinical factors. Document pulse by position where required and report concerning changes according to facility guidance.
Symptoms to Observe During Orthostatic Vital Signs
Symptoms are central to orthostatic vital signs nursing assessment. The numbers matter, but the patient’s experience and visible tolerance matter too.
Watch for:
- Dizziness
- Lightheadedness
- Weakness
- Faintness
- Blurred vision where relevant
- Nausea where relevant
- Pallor
- Diaphoresis
- Unsteadiness
- Near-fall behavior
- Shortness of breath where relevant
- Change in alertness or responsiveness
Symptoms such as dizziness and lightheadedness are subjective data because the patient reports them. Signs such as pallor, diaphoresis, swaying, or needing support are observable assessment findings. Nursing students should combine both.
If symptoms occur, prioritize safety and follow policy. Do not tell the patient to “push through” standing if they feel faint or unsafe. Seek instructor, preceptor, nurse, or provider guidance when unsure.
Factors That Can Affect Orthostatic Vital Signs
| Factor | How it may affect readings | Nursing consideration |
|---|---|---|
| Dehydration concerns | May be associated with position-related BP or pulse changes | Cluster with intake, output, mucous membranes, symptoms, and clinical context |
| Blood loss concerns | May affect BP, pulse, pallor, weakness, or dizziness | Report according to policy and patient condition |
| Medications | Some medications can affect BP, pulse, or position tolerance | Do not adjust medications; report concerns |
| Prolonged bed rest | May reduce position tolerance | Assist safely and follow mobility guidance |
| Age/frailty | May increase fall risk or symptom burden | Use safety precautions and compare with baseline |
| Autonomic dysfunction context | May affect BP and pulse response | Interpret with history, symptoms, and provider guidance |
| Activity level | Recent activity can raise pulse and BP | Consider rest period and policy timing |
| Pain | May increase pulse, BP, distress, and movement difficulty | Assess pain separately and document |
| Anxiety | May raise pulse and BP | Explain procedure and reassess if appropriate |
| Recent meals where relevant | May affect symptoms or BP in some patients | Consider timing and patient report |
| Fever or illness | May affect pulse, hydration, and weakness | Cluster with full assessment |
| Cuff size | Wrong cuff size can distort BP | Use correct cuff size |
| Arm position | Arm not at heart level may affect BP | Position correctly per policy |
| Timing between positions | Timing affects comparison | Follow facility protocol |
| Device accuracy | Automated devices may produce unexpected readings | Verify when required |
| Patient movement | Movement can distort BP and pulse readings | Reassess under better conditions when safe |
| Measurement technique | Poor technique can create misleading results | Use skills-lab and facility standards |
Orthostatic Vital Signs Chart for Nursing Students
| Item | What to check | Documentation reminder |
|---|---|---|
| Baseline vitals | Review recent BP, pulse, symptoms, and usual readings if available | Note comparison with baseline when relevant |
| Lying BP/pulse | Measure after required rest period according to policy | Document supine/lying BP, pulse, time |
| Sitting BP/pulse | Check tolerance, dizziness, weakness, balance, and required readings | Document sitting readings and symptoms if measured |
| Standing BP/pulse | Observe safety, balance, symptoms, BP, pulse, and timing | Document standing readings, timing, and patient response |
| Symptoms | Ask about dizziness, lightheadedness, weakness, faintness, nausea, blurred vision | Document patient’s words when useful |
| Timing | Follow facility timing between position changes | Include timing if required |
| Patient safety | Use assistance, gait belt, bed position, or support as required by policy | Document intolerance or assistance needed |
| Reassessment | Repeat questionable readings according to policy | Document reassessment values |
| Who was notified | Notify nurse, instructor, preceptor, or provider as required | Document notification per policy |
How to Document Orthostatic Vital Signs
Orthostatic vital signs documentation should be specific. Avoid vague documentation such as “orthostatics done” without values, positions, symptoms, or context.
Document:
- Position for each reading
- BP and pulse for each position measured
- Symptoms or absence of symptoms when required
- Timing according to policy
- Patient tolerance
- Safety concerns
- Reassessment if completed
- Notification according to policy
Documentation examples:
“Orthostatic VS obtained per policy: supine BP /, HR ___; sitting BP /, HR ___; standing BP /, HR ___; patient reported lightheadedness on standing; RN notified.”
“Patient denied dizziness during position changes; readings documented in flowsheet.”
“Standing reading stopped due to patient weakness and unsteadiness; patient assisted back to sitting; instructor and RN notified.”
“Orthostatic BP/pulse obtained lying and standing per order; patient tolerated position change without dizziness.”
Good documentation helps the care team understand what happened, what position the patient was in, whether symptoms occurred, and who was notified.
Orthostatic Vital Signs and Cue Clustering
Orthostatic readings should be clustered with the whole patient picture. Do not interpret one set of readings alone.
Cluster with:
- Baseline vital signs
- Current BP and pulse by position
- Dizziness or lightheadedness
- Weakness or faintness
- Hydration status
- Intake and output where relevant
- Recent falls
- Medications that may affect BP or pulse
- Blood loss concerns where relevant
- Pallor or diaphoresis
- Mental status
- Activity tolerance
- Recent procedures
- Pain level
- Caregiver or family report where relevant
Objective data include BP and pulse readings. Subjective data include dizziness, weakness, feeling faint, or “I feel like I might pass out.” Observable cues include swaying, pallor, diaphoresis, or needing support.
Example 1: Dizziness on Standing With BP/Pulse Change
Scenario: A patient reports dizziness after moving from lying to standing.
Objective cues: Standing BP and pulse differ from supine readings. Patient appears unsteady.
Subjective cues: Patient says, “I feel lightheaded.”
Possible nursing concern: Position-related intolerance may be present, but the student should not diagnose from one reading.
Appropriate student action: Ensure safety, assist the patient according to policy, reassess as directed, document readings by position and symptoms, and report to the nurse, instructor, or preceptor.
Example 2: Fall Risk Concern in an Older Adult
Scenario: An older adult had a recent fall and reports weakness when getting up.
Objective cues: Orthostatic readings are collected per policy. Patient needs support during standing.
Subjective cues: Patient reports feeling “wobbly” after standing.
Possible nursing concern: The cue cluster may suggest increased fall risk or poor position tolerance.
Appropriate student action: Maintain safety, document position-specific readings and symptoms, report according to facility guidance, and avoid independent treatment decisions.
Example 3: Reading Inconsistent With Symptoms or Poor Technique
Scenario: A patient has an unexpected standing BP reading, but the cuff slipped and the patient was moving.
Objective cues: Reading may be unreliable because measurement conditions were poor.
Subjective cues: Patient denies dizziness.
Possible nursing concern: The number may reflect technique error, but it still needs careful reassessment.
Appropriate student action: Check cuff placement and patient position, repeat per policy, document final reliable readings, and report if values or symptoms remain concerning.
Common Orthostatic Vital Signs Mistakes Nursing Students Make
| Mistake | Why it matters | Safer habit |
|---|---|---|
| Not documenting position | Readings cannot be compared accurately | Label supine, sitting, and standing values |
| Skipping symptoms | Symptoms may be clinically important even with borderline readings | Ask and document dizziness, weakness, faintness, or absence of symptoms |
| Rushing position changes | Symptoms may appear during transition | Follow facility timing and safety guidance |
| Using wrong cuff size | BP may be falsely high or low | Select correct cuff size |
| Not supporting patient safety during standing | Patient may become dizzy or fall | Use assistance and policy-based safety measures |
| Trusting one abnormal reading without reassessment | Poor technique can distort results | Recheck technique and reassess according to policy |
| Ignoring dizziness because numbers seem normal | Symptoms still matter | Report symptoms and document patient response |
| Comparing readings without considering timing | Timing affects interpretation | Follow protocol and document timing if required |
| Failing to report concerning symptoms | Delayed communication may affect safety | Notify nurse/instructor/preceptor according to policy |
| Documenting “orthostatics positive/negative” without values | The care team needs objective data and context | Record values, positions, symptoms, and notification |
| Confusing routine BP with orthostatic assessment | One-position BP does not show position response | Compare readings across positions |
When to Report Orthostatic Vital Signs
Report orthostatic vital signs according to facility parameters, instructor or preceptor guidance, provider orders, early warning systems if used, and patient condition.
Report when there are:
- Dizziness, lightheadedness, faintness, or weakness during position change
- Sudden changes from baseline
- Worsening trends
- Readings outside assigned parameters
- Falls risk or unsteadiness
- Pallor, diaphoresis, or near-fall behavior
- Readings inconsistent with patient appearance
- Symptoms despite values that appear acceptable
- Poor tolerance of sitting or standing
- Uncertainty about technique or interpretation
Escalate uncertainty rather than guessing. Nursing students should not diagnose orthostatic hypotension from one set of readings or provide treatment instructions. The student’s role is to assess within scope, maintain safety, document clearly, and report according to clinical guidance.
How to Study Orthostatic Vital Signs for Nursing School
Start with routine vital signs. Make sure you understand blood pressure, pulse, baseline comparison, trends, and documentation. Then study how position changes affect interpretation.
Useful study strategies:
- Learn why lying, sitting, and standing positions matter.
- Practice organizing readings by position.
- Memorize what must be documented.
- Study symptoms linked to position changes.
- Practice cue clustering with short scenarios.
- Review facility or instructor expectations before clinical.
- Avoid memorizing thresholds without context.
- Practice writing documentation examples.
- Ask your instructor how your program wants orthostatic readings reported.
- Remember that safety comes before completing the sequence.
Orthostatic vital signs become easier when students stop viewing them as “extra blood pressures” and start viewing them as a position-change assessment.
When to Ask for Help With Orthostatic Vital Signs Assignments
Students may need help with nursing assessment assignments, case studies, documentation examples, care plans, clinical reflections, or vital sign interpretation questions. Support can help with organizing answers, explaining cue clustering, and applying nursing assessment concepts to assignment instructions.
For coursework support, students can review nursing assignment help, nursing case study help, or healthcare assignment help. These links belong here because this section focuses on academic guidance, not clinical decision-making.
FAQs About Orthostatic Vital Signs
1. What are orthostatic vital signs?
Orthostatic vital signs are blood pressure and pulse measurements taken across position changes, commonly lying, sitting, and standing depending on facility policy.
2. Why are orthostatic vital signs taken?
They may be taken to assess position-related changes in blood pressure, pulse, and symptoms such as dizziness, lightheadedness, weakness, faintness, or falls risk.
3. What positions are used for orthostatic vital signs?
Common positions include lying, sitting, and standing. Some policies use lying and standing only. Students should follow facility and instructor guidance.
4. What vital signs are measured during orthostatic assessment?
Blood pressure and pulse are usually central. Symptoms and patient tolerance are also observed and documented.
5. What symptoms should nurses watch for during orthostatic vital signs?
Watch for dizziness, lightheadedness, weakness, faintness, blurred vision, nausea, pallor, diaphoresis, unsteadiness, and near-fall behavior.
6. How are orthostatic vital signs documented?
Document readings by position, including BP and pulse, timing if required, symptoms or absence of symptoms, patient tolerance, reassessment, and who was notified when required.
7. Can orthostatic vital signs diagnose orthostatic hypotension?
A single orthostatic reading should not be used by a student to diagnose a condition. Orthostatic findings must be interpreted with symptoms, baseline, technique, patient condition, provider guidance, and facility policy.
8. What can affect orthostatic vital signs?
Hydration status, medications, blood loss concerns, prolonged bed rest, age, frailty, autonomic issues, pain, anxiety, recent activity, cuff size, arm position, timing, device accuracy, and measurement technique can affect readings.
9. When should nursing students report orthostatic vital signs?
Report symptoms, sudden changes, worsening trends, readings outside assigned parameters, fall risk, poor standing tolerance, or any uncertainty according to facility policy and instructor or preceptor guidance.
10. How are orthostatic vital signs different from routine vital signs?
Routine vital signs measure current status at one time or position. Orthostatic vital signs compare blood pressure, pulse, and symptoms across position changes.
Concluding Thoughts on Orthostatic Vital Signs
Orthostatic vital signs are position-change assessments, not routine one-position readings. Blood pressure, pulse, symptoms, baseline, technique, timing, and safety all matter.
Nursing students should document readings by position, observe symptoms carefully, compare findings with baseline and patient condition, and report concerning findings according to policy. A patient’s dizziness, weakness, unsteadiness, or near-fall behavior should not be ignored because a number appears acceptable.
Orthostatic vital sign interpretation must follow facility policy, instructor guidance, provider orders, patient condition, scope of practice, and clinical judgment.
If students need help with orthostatic vital signs assignments, nursing assessment case studies, clinical reflection, documentation examples, or care plan interpretation, they can upload their instructions and rubric for academic guidance.
References
Centers for Disease Control and Prevention. (2024). Measuring orthostatic blood pressure. https://www.cdc.gov/steadi/media/pdfs/STEADI-Assessment-MeasuringBP-508.pdf
Centers for Disease Control and Prevention. (2025). Clinical resources: STEADI—Older adult fall prevention. https://www.cdc.gov/steadi/hcp/clinical-resources/index.html
Ernstmeyer, K., & Christman, E. (Eds.). (2023). Nursing skills: Blood pressure basics (2nd ed.). Wisconsin Technical College System/Open RN. https://wtcs.pressbooks.pub/nursingskills/chapter/3-2-blood-pressure-basics/
Merck Manual Consumer Version. (2024). Low blood pressure. https://www.merckmanuals.com/home/heart-and-blood-vessel-disorders/low-blood-pressure-and-shock/low-blood-pressure
MSD Manual Professional Edition. (2024). Orthostatic hypotension. https://www.msdmanuals.com/professional/cardiovascular-disorders/symptoms-of-cardiovascular-disorders/orthostatic-hypotension
Ringer, M., Lappin, S. L., & Farrar, J. (2025). Orthostatic hypotension. StatPearls/NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK448192/
Sapra, A., Malik, A., & Bhandari, P. (2023). Vital sign assessment. StatPearls/NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK553213/