Pediatric vital signs help nursing students assess a child’s physiological status, but they are not interpreted the same way as adult vital signs. Many students first learn adult temperature, pulse, respirations, blood pressure, and oxygen saturation, then feel unsure when pediatric values change by age, crying, fever, activity, anxiety, respiratory effort, and developmental stage.
This guide explains pediatric vital signs by age, including temperature, heart rate, respiratory rate, blood pressure, oxygen saturation, pain assessment, documentation, common errors, cue clustering, and when to report changes. This guide is for nursing education and pediatric assessment learning only. Pediatric vital sign assessment and response must follow facility policy, instructor guidance, provider orders, patient condition, scope of practice, and clinical judgment.
For students who need the broader foundation first, our complete vital signs guide explains general vital signs assessment, trends, documentation, pain assessment, and cue clustering across nursing contexts. This article stays focused on pediatric vital signs and how nursing students should interpret them safely. The article follows the detailed writing brief supplied for the pediatric vital signs supporting article.
Quick Answer: What Are Pediatric Vital Signs?
Pediatric vital signs are measurable indicators used to assess a child’s physiological status.
They commonly include temperature, heart rate or pulse, respiratory rate, blood pressure, and oxygen saturation. Traditional vital signs include temperature, pulse, blood pressure, and respiratory rate, while pulse oximetry is often used to add useful cardiopulmonary context (Sapra et al., 2023).
Normal pediatric vital signs vary by age, activity, fever, crying, anxiety, baseline, and measurement technique.
Infants and younger children often have faster heart and respiratory rates than adults.
A single reading should be interpreted with the child’s full condition, not in isolation.
Nursing students should compare readings with age-based expectations, baseline, symptoms, trends, and facility parameters.
What Makes Pediatric Vital Signs Different From Adult Vital Signs?
Children are not simply small adults. Their expected heart rate, respiratory rate, blood pressure, behavior, and response to illness or stress vary by age and development. MedlinePlus notes that normal vital signs change with age, weight, exercise capacity, sex, and overall health, which is why adult ranges should not be copied into pediatric assessment (MedlinePlus, 2025).
Younger children usually have faster heart and respiratory rates than adults. An infant may have a pulse that looks “high” beside an adult range but may still fit pediatric expectations. A school-age child or adolescent may have values closer to adult ranges, but students should still interpret the findings using the child’s age, size, baseline, symptoms, and setting.
Pediatric readings are also more easily affected by behavior and technique. Crying, fear, recent play, fever, pain, movement, poor cuff fit, body position, probe placement, and device artifact can change the reading. This does not mean students should dismiss abnormal values. It means they should ask: Was the child calm or the cuff correct? Was the probe reading reliable? Did the child work harder to breathe? Does the reading match the child’s appearance?
A useful pediatric habit is to interpret the number with the child, not away from the child. Look at the child’s color, alertness, work of breathing, posture, hydration cues, pain behavior, activity level, parent or caregiver report, and trend over time.
Pediatric Vital Signs Chart by Age
The following pediatric vital signs chart gives practical age-based ranges for nursing-student learning. Ranges vary by source, institution, patient condition, baseline, activity, and measurement method. The Royal Children’s Hospital guideline specifically warns that published pediatric ranges differ and that patterns of change are often as important as the threshold itself (Royal Children’s Hospital Melbourne, 2023).
Newborn vital signs are not merged into this chart because newborns have transitional circulation, thermoregulation, feeding, respiratory, and adaptation considerations that deserve a separate focused guide.
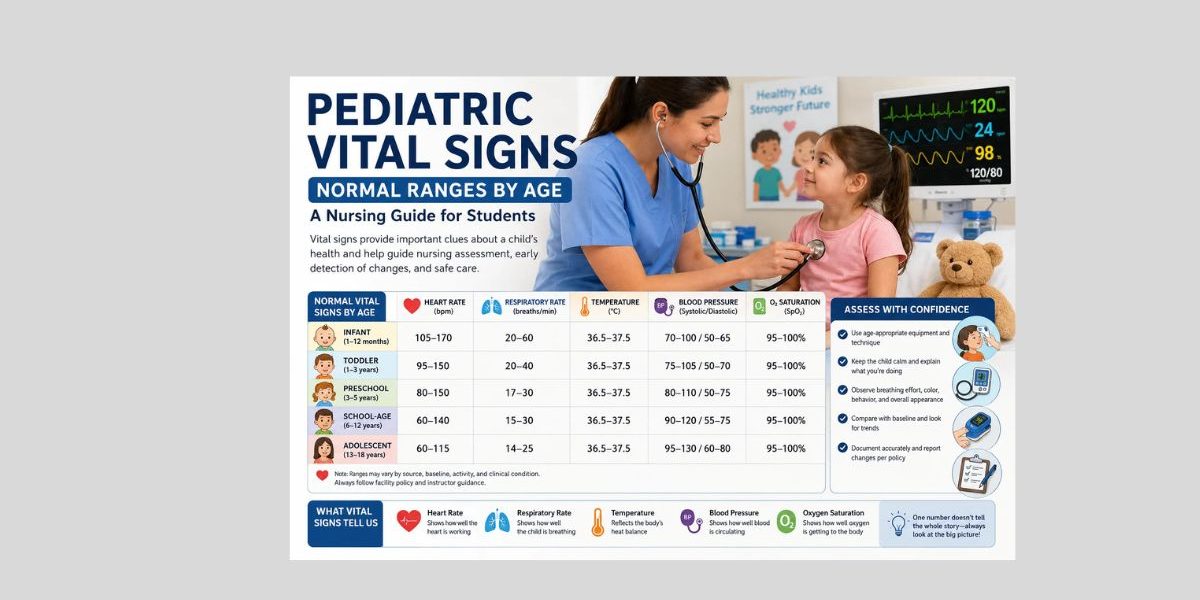
| Age group | Heart rate/pulse | Respiratory rate | Blood pressure overview | Oxygen saturation overview | Nursing notes |
|---|---|---|---|---|---|
| Infant, beyond immediate newborn period | About 105–170 bpm, depending on age and state | About 20–60/min, depending on age | Systolic BP often lower than older children; use age, size, and policy-based parameters | Interpret with probe quality, color, breathing effort, oxygen use, and baseline | Feeding, crying, fever, sleep, movement, and respiratory effort can strongly affect readings |
| Toddler | About 95–150 bpm | About 20–40/min | Correct cuff size matters; anxiety and movement can distort readings | Watch motion artifact and probe placement | Toddlers may resist assessment, cry, or move, so document context |
| Preschool child | About 80–150 bpm | About 17–30/min | Systolic BP gradually increases with age and size | Interpret with respiratory effort and appearance | Use simple explanations; assess before the child becomes distressed when appropriate |
| School-age child | About 60–140 bpm across the range, lower with increasing age | About 15–30/min | BP interpretation depends on age, height, sex, and technique | Compare SpO2 with respiratory pattern, effort, color, and symptoms | More cooperative, but fever, pain, activity, and anxiety still matter |
| Adolescent | About 60–115 bpm | About 14–25/min | Values may approach adult patterns, but context still matters | Interpret with symptoms, activity, perfusion, and device accuracy | Privacy, anxiety, pain, hydration, medications, and chronic conditions may affect readings |
These ranges are learning guides, not diagnostic rules. For example, a heart rate within an “acceptable” age range may still be concerning if it is rising steadily, very different from the child’s baseline, or paired with distress. RCH emphasizes repeated observations, previous measurements, and clinical context when interpreting pediatric physiological variables (Royal Children’s Hospital Melbourne, 2023).
Infant Vital Signs
Infant vital signs beyond the immediate newborn period often look fast compared with adult values. Infants have higher expected heart and respiratory rates, and their readings can shift with feeding, crying, sleep, fever, movement, and distress.
For nursing students, the most important point is not only the number. It is the number plus the infant’s appearance. Observe color, alertness, feeding behavior, tone, respiratory effort, cry strength, hydration cues, caregiver concern, and whether the infant calms after rest.
Respiratory assessment is especially important. An infant’s respiratory rate may rise with crying or fever, but increased work of breathing, retractions, nasal flaring, grunting, poor feeding, color change, or lethargy should not be ignored. A focused respiratory assessment includes vital signs, breathing pattern, skin color, respiratory status, and other assessment findings (Ernstmeyer & Christman, 2021).
Documentation should include the value, time, route or site, activity state, and relevant context. For example, “HR 148 bpm, apical, regular, infant crying before assessment; reassessed after calming per instructor guidance.”
Toddler Vital Signs
Toddler vital signs can be difficult because toddlers may resist assessment, cry, hide, move, or become fearful. Their readings may rise because of anxiety, play, fever, pain, or lack of cooperation. This is why nursing students should avoid grabbing quick numbers without observing the child’s behavior and context.
Where policy allows, observe the toddler before touching. Note breathing pattern, color, posture, activity, and level of distress. A caregiver’s presence may help the child feel safer, although students should follow facility and instructor expectations.
A toddler’s pulse and respirations should be interpreted with behavior. A crying toddler may have an elevated pulse, but a persistent elevated rate after rest, a worsening trend, or respiratory effort should prompt reassessment and reporting according to policy.
Documentation should not hide the context. “RR 36/min while crying” is more useful than “RR 36” alone. If the child calms and the reading changes, document the reassessment according to clinical expectations.
Preschool Vital Signs
Preschool children may understand simple explanations but may still fear equipment, pain, or separation from caregivers. They may cooperate better when students use short, concrete explanations such as, “This cuff gives your arm a hug,” but students should avoid making promises that are not accurate.
Movement, anxiety, and recent activity can affect preschool vital signs. A preschool child who has just been running, crying, or resisting may have a higher pulse and respiratory rate than a child resting quietly. The student’s job is to recognize the context and decide whether the reading should be repeated after rest according to policy.
Blood pressure measurement requires correct cuff size and positioning. Poor cuff fit can produce misleading readings. For pediatric blood pressure, the cuff bladder width should be about 40% of mid-upper-arm circumference and the length should cover about 80% to 100% of the arm circumference (MSD Manual Professional Edition, 2025).
Documentation should include the reading and any relevant context: “BP 92/58 mmHg, right arm, child seated, child calm during reading.”
School-Age Vital Signs
School-age children usually cooperate more with pediatric clinical skills, but students should still assess context. Fever, pain, anxiety, dehydration, activity, medications, and respiratory symptoms can affect vital signs.
At this stage, children may be able to describe symptoms more clearly. Students should connect objective data with subjective reports. For example, a school-age child may report chest tightness, dizziness, pain, or feeling “too tired,” while the student also observes respiratory rate, pulse, color, posture, and oxygen saturation. If you have an article on subjective and objective data, this is a natural place to internally link it because pediatric vital signs are objective data, while the child’s symptoms and caregiver report add subjective context.
School-age documentation should be clear, complete, and specific. Avoid vague phrases such as “vitals okay.” Instead, document values, timing, site or route, and assessment context.
Adolescent Vital Signs
Adolescent values may approach adult ranges, but nursing students should not assume every adolescent vital sign can be interpreted exactly like an adult reading. Age, body size, pain, anxiety, privacy concerns, hydration, activity, caffeine or nicotine exposure where relevant, medications, chronic conditions, and emotional distress can affect readings.
Adolescents may also underreport symptoms because of embarrassment, fear, or desire for privacy. Students should use professional communication, protect dignity, and follow facility rules about caregiver presence and adolescent confidentiality.
When documenting adolescent vital signs, include the same essentials: value, unit, time, route or site, position where relevant, oxygen use if present, pain score or tool if used, and any reassessment or reporting.
Pediatric Temperature Assessment
Pediatric temperature reflects body heat balance and may change with infection, inflammation, environment, activity, clothing, recent bath, time of day, or medication effects. Temperature route matters. Oral, tympanic, temporal, axillary, and rectal routes may produce different readings and may be used differently depending on age, setting, policy, equipment, and contraindications.
Johns Hopkins Medicine explains that body temperature can vary with recent activity, food and fluid intake, time of day, and route; it also notes that rectal temperatures tend to be higher than oral readings, while axillary temperatures tend to be lower (Johns Hopkins Medicine, 2025).
For nursing students, the safest approach is to document the exact route. “Temperature 38.1°C” is incomplete if the route matters. “Temperature 38.1°C tympanic at 0900; child crying before reading” gives better context.
Do not treat the temperature value as a diagnosis. Fever may be associated with infection or other causes, while low temperature may also need attention depending on age, condition, and setting. Students should reassess, document, and report according to facility policy, instructor guidance, provider orders, and patient condition.
Pediatric Heart Rate and Pulse Assessment
Pediatric heart rate, or pulse rate, is the number of heartbeats per minute. In children, pulse can change quickly with crying, fear, fever, pain, activity, dehydration, medications, and illness.
Assessment should include more than the number when the skill requires it. Students may need to note rhythm, strength, site, and whether the pulse was apical or peripheral. In some pediatric learning contexts, an apical pulse may be preferred for younger children or when accuracy is important, but students should follow skills-lab instructions and facility policy.
A high pulse after running or crying may not mean the same thing as a high pulse at rest with lethargy, fever, poor intake, or respiratory distress. The cue cluster matters.
Documentation examples:
“HR 118 bpm, apical, regular, after rest.”
“Pulse 132 bpm radial, child anxious during assessment; instructor notified per clinical guidance.”
Pediatric Respiratory Rate Assessment
Pediatric respiratory rate is one of the most important pediatric vital signs because children can show respiratory changes early. Younger children often breathe faster than adults, so adult respiratory ranges should not be applied to infants, toddlers, or preschoolers.
Count respirations carefully. Do not estimate from the monitor alone when the skill requires direct assessment. Observe chest or abdominal movement, rhythm, effort, and pattern. Respiratory rate may increase with fever, illness, or distress, and Johns Hopkins Medicine notes that respiratory assessment should include whether the person has difficulty breathing (Johns Hopkins Medicine, 2025).
Also observe work of breathing. Look for retractions, nasal flaring, grunting, wheezing, posture, color, fatigue, and ability to speak, feed, or play when age appropriate. Interpret respiratory rate together with oxygen saturation, appearance, and overall condition.
Documentation examples:
“RR 32/min, mild increased work of breathing noted.”
“RR 28/min, regular, child resting quietly.”
“RR 40/min after crying; reassessed after rest per instructor guidance.”
Pediatric Blood Pressure Assessment
Pediatric blood pressure varies by age, sex, height, size, position, activity, anxiety, and technique. It is not interpreted as simply as adult blood pressure. In children under 13, BP interpretation can require age, sex, and height percentiles; adolescents 13 and older may be interpreted with categories that align more closely with adult definitions, depending on the guideline used (MSD Manual Professional Edition, 2025).
Correct cuff size is essential. A cuff that is too small can falsely elevate the reading, while a cuff that is too large can give a falsely low reading. The University of Iowa pediatric vital signs protocol also notes that ideal cuff bladder length is about 80% of arm circumference and width at least 40% of arm circumference (University of Iowa Health Care, 2017).
Position matters. The child should be as calm and appropriately positioned as possible. Movement, unsupported posture, crossed legs in older children, an arm not at heart level, or clothing under the cuff may affect accuracy.
Automated blood pressure readings may need verification when unexpected. The MSD Manual notes that oscillometric measurements are often higher than auscultatory measurements and that elevated readings may need confirmation by auscultation (MSD Manual Professional Edition, 2025).
Documentation examples:
“BP 104/62 mmHg, right arm, child seated, appropriate cuff size.”
“BP 118/70 mmHg automated; child moving during reading; repeated manually per instructor guidance.”
Pediatric Oxygen Saturation Assessment
Pediatric oxygen saturation, or pediatric SpO2, estimates the percentage of hemoglobin saturated with oxygen. It is useful, but it must be interpreted with the child’s appearance and respiratory assessment.
Signal quality matters. Poor probe placement, motion, cold extremities, poor perfusion, nail products, device fit, and child movement can affect the reading. Students should not document a questionable number without checking the child and the device.
Interpret SpO2 with respiratory effort, color, level of alertness, work of breathing, oxygen device if present, symptoms, and trend. A low reading with a poor waveform or loose probe may require probe repositioning and reassessment. A low reading with increased work of breathing, color change, or altered behavior requires prompt reporting according to facility policy and clinical guidance.
Documentation examples:
“SpO2 96% on room air; probe repositioned before final reading.”
“SpO2 94% on room air, mild nasal flaring observed; reported to assigned nurse per policy.”
Do not use this article as oxygen administration guidance. Oxygen therapy and device changes must follow provider orders, facility policy, scope of practice, and instructor or preceptor direction.
Pediatric Pain Assessment and Vital Signs
Pain assessment matters in pediatric nursing, but pain should not be treated as a simple universal vital sign in all settings. Pain is subjective and should be assessed using age-appropriate tools and behavioral cues.
Infants and young children may show pain through crying, facial expression, guarding, sleep changes, decreased feeding, restlessness, irritability, or decreased movement. Older children and adolescents may use a numeric, faces, or other facility-approved pain scale depending on age and communication ability.
Pain can affect pulse, respirations, blood pressure, sleep, behavior, and distress. However, normal vital signs do not prove that pain is absent. Students should document the pain scale or tool, score or behavior, location if known, caregiver input when relevant, and reassessment according to policy.
Documentation example:
“Pain 4/10 using age-appropriate scale; parent present; reassessment completed per facility policy.”
Factors That Affect Pediatric Vital Signs
| Factor | Vital signs affected | Pediatric nursing consideration |
|---|---|---|
| Age | HR, RR, BP | Compare with pediatric age group, not adult ranges |
| Crying | HR, RR, BP, SpO2 artifact | Note context and reassess when calm if appropriate |
| Anxiety or fear | HR, RR, BP | Use age-appropriate communication and caregiver support when allowed |
| Fever | Temperature, HR, RR | Interpret with symptoms, hydration, behavior, and trend |
| Activity or play | HR, RR, BP | Rest before measurement when policy requires |
| Sleep | HR, RR, BP | Sleeping values may differ from awake values |
| Pain | HR, RR, BP, behavior | Use age-appropriate pain tools and behavioral cues |
| Dehydration | HR, BP, perfusion cues | Cluster with intake, output, mucous membranes, and overall appearance |
| Medications | HR, RR, BP, temperature | Consider recent prescribed medications within scope and report concerns |
| Respiratory illness | RR, SpO2, HR | Observe work of breathing, color, posture, and fatigue |
| Oxygen therapy | SpO2, RR, work of breathing | Document device and flow if required by policy |
| Body position | BP, RR, SpO2 | Document position if clinically relevant |
| Cuff size | BP | Wrong cuff size can distort blood pressure readings |
| Device placement | SpO2, BP, temperature | Check placement before accepting unexpected readings |
| Recent procedures | HR, RR, BP, pain | Consider stress, pain, sedation, or procedure-related context |
| Developmental stage | All readings indirectly | Cooperation and fear affect measurement accuracy |
| Parent/caregiver presence | HR, RR, behavior | May calm the child and improve assessment accuracy |
| Measurement technique | All vital signs | Use correct route, site, timing, equipment, and documentation |
Pediatric Vital Sign Trends vs One-Time Readings
One pediatric vital sign reading can be misleading. A child may cry during one reading, move during a blood pressure measurement, or have a poor pulse oximeter signal. However, a trend can show whether the child is improving, worsening, or changing.
Trends are especially important in pediatric nursing. A heart rate that steadily rises, a respiratory rate that increases over several checks, or an SpO2 that gradually falls may matter even before a single value looks extreme. RCH specifically states that patterns of change are often more important than the value itself and recommends repeated observations and comparison with previous measurements (Royal Children’s Hospital Melbourne, 2023).
Students should compare the reading with the child’s baseline if available. Ask whether the child was resting, crying, febrile, in pain, recently active, receiving oxygen, or recently assessed after a procedure.
A value within the normal pediatric vital signs chart may still matter if it is far from that child’s baseline or paired with concerning symptoms. A value outside the expected range may require reassessment if technique or context may have affected it. Either way, students should avoid guessing and should report concerning changes according to instructor, preceptor, nurse, provider, or facility guidance.
How to Take Pediatric Vital Signs Accurately
Accurate pediatric vital signs require preparation, correct equipment, child-friendly communication, and careful interpretation.
Use this practical checklist:
- Confirm the child’s age and relevant baseline if available.
- Review facility parameters, provider orders, and instructor expectations.
- Prepare the child and caregiver using age-appropriate language.
- Use the correct thermometer route, blood pressure cuff, pulse site, and SpO2 probe.
- Reduce anxiety where possible.
- Observe breathing, color, posture, behavior, and distress before disturbing the child when appropriate.
- Count respirations carefully instead of estimating.
- Recheck unexpected readings when technique, movement, or device artifact may be involved.
- Compare findings with age expectations, baseline, symptoms, and trends.
- Document values, units, route or site, time, context, and reporting.
This checklist does not replace pediatric skills-lab instruction. Students should follow the procedure taught by their program and facility.
Manual vs Automated Pediatric Vital Signs
Automated devices are useful in pediatric settings, but they are not perfect. Movement, poor cuff size, loose probe placement, poor perfusion, device error, and child distress can affect readings. Johns Hopkins Medicine notes that body movement or irregular heart rhythm can affect digital blood pressure monitor accuracy (Johns Hopkins Medicine, 2025).
Manual assessment remains important for verification and skills learning. Nursing students should not copy unexpected monitor readings without checking whether the child was moving, crying, poorly positioned, or attached to a loose sensor.
A safe student habit is simple: check the child first, then check the device. If the number does not match the child’s presentation, reassess according to policy and ask for help.
Abnormal Pediatric Vital Signs: How Nursing Students Should Think
Abnormal pediatric vital signs may mean several things. A value may be outside the expected age range. It may be different from baseline or worsening over time. Still, it may be inconsistent with the child’s appearance. It may be paired with symptoms such as respiratory distress, fever, pain, lethargy, poor feeding, dehydration cues, or caregiver concern.
Do not interpret one number alone. Cluster cues.
For example, a high respiratory rate with increased work of breathing may suggest the child needs prompt reassessment and reporting. A fever with elevated heart rate may reflect the body’s response to illness, pain, distress, or dehydration risk, but the student should not diagnose the cause from vital signs alone. A low oxygen saturation reading with a poor probe signal may require repositioning and reassessment, while a low reading with color change or increased work of breathing should be reported according to facility policy.
A “normal” chart range can also be misleading. If a child appears lethargic, pale, distressed, or very different from baseline, students should not ignore the child because the vital sign fits a table.
Pediatric Vital Signs Documentation
Pediatric vital signs documentation should be clear, objective, complete, and contextual. Document what was measured, how it was measured, and what mattered clinically.
Include:
- Value and unit
- Time
- Route or site
- Position if relevant
- Oxygen device and flow if applicable and required by policy
- Pain scale or behavioral pain tool if used
- Child activity, crying, sleep, or distress if relevant
- Reassessment when required
- Abnormal findings and who was notified according to policy
Examples:
“Temperature 38.1°C tympanic at 0900; child crying before reading.”
“HR 118 bpm, apical, regular, after rest.”
“RR 32/min, mild increased work of breathing noted.”
“SpO2 96% on room air; probe repositioned before final reading.”
“Pain 4/10 using age-appropriate scale; parent present.”
Avoid vague documentation such as “vitals stable” unless your facility specifically allows it and the actual values are recorded elsewhere. Use facility-approved abbreviations only.
Common Pediatric Vital Signs Mistakes Nursing Students Make
| Mistake | Why it matters | Safer habit |
|---|---|---|
| Using adult ranges for children | Pediatric HR, RR, and BP differ by age | Use pediatric age-based references |
| Confusing newborn and pediatric ranges | Newborn transition has separate considerations | Keep newborn vital signs separate |
| Not considering crying or activity | Distress can raise HR, RR, and BP | Document context and reassess if appropriate |
| Using the wrong cuff size | BP may be falsely high or low | Select cuff based on arm size |
| Counting respirations inaccurately | RR is a key pediatric cue | Count carefully and observe effort |
| Ignoring respiratory effort | A number alone may miss distress | Assess retractions, flaring, color, posture, and fatigue |
| Trusting monitor readings without checking the child | Devices can show artifact | Assess the child and verify unexpected readings |
| Failing to reassess unexpected values | One reading may be affected by technique | Repeat according to policy |
| Documenting without context | The chart may not explain why a value changed | Add route, site, activity, and reassessment |
| Ignoring parent/caregiver report | Caregivers may notice subtle changes | Include relevant caregiver concerns |
| Missing trends | A worsening pattern can matter | Compare with previous readings |
| Not reporting concerning changes | Delay can affect safety | Report according to policy and instructor guidance |
Pediatric Vital Signs and Cue Clustering Examples
Example 1: Fever and Tachycardia
Scenario: A school-age child has a temperature of 38.4°C and HR 128 bpm.
Objective vital sign cues: Elevated temperature and heart rate for context.
Subjective/caregiver cues: Caregiver reports the child has been tired and drinking less.
Other assessment cues: Child appears flushed and less playful than earlier.
Possible nursing concern: The elevated heart rate may be associated with fever, distress, pain, hydration status, or illness, but the student should not diagnose the cause.
Appropriate student action: Reassess as instructed, document temperature route and heart rate site, report findings to the nurse or instructor according to policy, and continue cue clustering.
Example 2: Increased Respiratory Rate With Work of Breathing
Scenario: A toddler has RR 42/min and mild retractions after being calm for several minutes.
Objective vital sign cues: Respiratory rate is high for age context, with increased work of breathing.
Subjective/caregiver cues: Caregiver says the child “has not been breathing like usual.”
Other assessment cues: Nasal flaring, reduced play, and mild fatigue.
Possible nursing concern: The cue cluster may suggest respiratory compromise or worsening respiratory status.
Appropriate student action: Reassess measurement accuracy, document respiratory effort, and report promptly to the assigned nurse, instructor, or preceptor according to facility guidance.
Example 3: Anxiety-Related Elevated Pulse
Scenario: A preschool child cries when the student approaches with equipment. HR is 142 bpm.
Objective vital sign cues: Heart rate is elevated in the moment.
Subjective/caregiver cues: Caregiver states the child becomes fearful during assessments.
Other assessment cues: Child is crying, pulling away, and calming when caregiver holds their hand.
Possible nursing concern: Anxiety may be contributing to the elevated pulse, but the student should still consider fever, pain, and other cues.
Appropriate student action: Use age-appropriate communication, allow calming when appropriate, reassess according to instructor guidance, and document the context.
Example 4: Low SpO2 Reading With Poor Probe Placement
Scenario: An infant’s SpO2 briefly reads 88%, but the probe is loose and the infant is kicking.
Objective vital sign cues: Low displayed SpO2 with poor signal quality.
Subjective/caregiver cues: Caregiver says the infant has been active and feeding normally.
Other assessment cues: Color appears normal, no obvious increased work of breathing, probe not secure.
Possible nursing concern: The reading may be artifact, but true oxygen desaturation must not be dismissed without reassessment.
Appropriate student action: Check probe placement, reassess according to policy, observe respiratory effort and color, document final reliable reading, and report concerns or persistent abnormal values.
When to Report Pediatric Vital Signs
Report pediatric vital signs according to facility parameters, instructor or preceptor guidance, provider orders, early warning systems if used, and the child’s condition.
Students should report:
- Sudden changes
- Worsening trends
- Readings outside assigned parameters
- Readings inconsistent with the child’s presentation
- Vital signs that do not match the child’s baseline
- Respiratory distress cues
- Concerning caregiver reports
- Repeated unexpected readings
- Device readings that remain abnormal after reassessment
- Any uncertainty about interpretation
Escalate uncertainty rather than guessing. A student does not need to diagnose the problem before asking for help. The safer approach is to reassess, document accurately, and communicate the concern using objective findings and relevant context.
How to Study Pediatric Vital Signs for Nursing School
Start by learning adult ranges, then deliberately separate pediatric ranges by age. Do not memorize one “child normal” number for every child.
Use these study strategies:
- Learn infant, toddler, preschool, school-age, and adolescent patterns separately.
- Keep newborn vital signs separate from pediatric vital signs.
- Practice reading pediatric charts by age group.
- Study how fever, crying, activity, pain, anxiety, and sleep affect readings.
- Practice documentation examples.
- Use pediatric case scenarios to cluster cues.
- Review cuff-size and probe-placement errors.
- Practice explaining when to reassess.
- Ask instructors to clarify facility-specific reporting parameters.
Pediatric vital signs become easier when students stop memorizing isolated numbers and begin asking, “Does this value fit this child, at this age, in this condition, at this time?”
When to Ask for Help With Pediatric Vital Signs Assignments
Students may need help with pediatric assessment assignments, case studies, documentation examples, clinical reflections, care plans, or vital signs interpretation questions. Support can help you organize your answers, explain cue clustering, apply pediatric nursing assessment concepts, and connect objective findings with subjective child or caregiver reports.
If your assignment involves pediatric clinical judgment, documentation, or a case study, you can review our nursing assignment help, nursing case study help, or healthcare assignment help pages for academic guidance. Use these support pages near assignment-related sections only, not as replacements for clinical instruction.
FAQs About Pediatric Vital Signs
1. What are pediatric vital signs?
Pediatric vital signs are measurements used to assess a child’s physiological status. They commonly include temperature, heart rate or pulse, respiratory rate, blood pressure, and oxygen saturation.
2. What are normal pediatric vital signs by age?
Normal pediatric vital signs vary by age group. Infants and toddlers usually have faster heart and respiratory rates than older children and adolescents. Ranges also vary by source, baseline, activity, fever, crying, condition, and measurement technique.
3. How are pediatric vital signs different from adult vital signs?
Pediatric values are more age-dependent. Younger children often have faster pulse and respiratory rates, and pediatric blood pressure depends strongly on age, size, sex, and height. Children may also be more affected by crying, fear, movement, and cooperation.
4. What is a normal pediatric heart rate?
A normal pediatric heart rate depends on age, activity, sleep, fever, pain, anxiety, and baseline. Infants usually have higher expected heart rates than school-age children and adolescents.
5. What is a normal pediatric respiratory rate?
A normal pediatric respiratory rate also depends on age. Infants and young children breathe faster than adults. Nursing students should count carefully and observe work of breathing, not just the number.
6. Why does cuff size matter for pediatric blood pressure?
Cuff size matters because a cuff that is too small can falsely raise blood pressure, while a cuff that is too large can falsely lower it. Pediatric BP measurement should use a cuff matched to the child’s arm size (MSD Manual Professional Edition, 2025).
7. How does crying affect pediatric vital signs?
Crying can increase heart rate, respiratory rate, and sometimes blood pressure. It can also interfere with oxygen saturation readings because of movement. Students should document the context and reassess when appropriate.
8. How should pediatric vital signs be documented?
Document the value, unit, time, route or site, position if relevant, oxygen device if present, pain tool if used, child activity or crying if relevant, reassessment, and who was notified for concerning findings.
9. When should nursing students report pediatric vital signs?
Students should report readings outside assigned parameters, sudden changes, worsening trends, symptoms, respiratory distress cues, readings that do not match the child’s baseline, or any uncertainty according to facility policy and instructor or preceptor guidance.
10. Are newborn vital signs the same as pediatric vital signs?
No. Newborn vital signs have unique transitional and thermoregulation considerations. Newborns should be addressed in a separate focused guide rather than merged completely with broader pediatric vital signs.
Final Thoughts on Pediatric Vital Signs
Pediatric vital signs require age-based interpretation. Normal ranges are only a starting point. Trends, symptoms, crying, fever, activity level, pain, technique, baseline, caregiver reports, and overall appearance all matter.
Nursing students should focus on accurate measurement, safe documentation, reassessment, cue clustering, and timely reporting. A pediatric vital signs chart can guide learning, but it should never replace clinical judgment, facility policy, instructor guidance, provider orders, or scope of practice.
If students need help with pediatric vital signs assignments, pediatric nursing case studies, clinical reflections, documentation examples, or care plan interpretation, they can upload their instructions and rubric for academic guidance.
References
Ernstmeyer, K., & Christman, E. (Eds.). (2021). Nursing skills: Chapter 10 respiratory assessment. Open RN/NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK593192/
Johns Hopkins Medicine. (2025). Vital signs (body temperature, pulse rate, respiration rate, blood pressure). https://www.hopkinsmedicine.org/health/conditions-and-diseases/vital-signs-body-temperature-pulse-rate-respiration-rate-blood-pressure
MedlinePlus. (2025). Vital signs. U.S. National Library of Medicine. https://medlineplus.gov/ency/article/002341.htm
MSD Manual Professional Edition. (2025). Hypertension in children. https://www.msdmanuals.com/professional/pediatrics/hypertension-in-children/hypertension-in-children
Royal Children’s Hospital Melbourne. (2023). Clinical practice guidelines: Acceptable ranges for physiological variables. https://www.rch.org.au/clinicalguide/guideline_index/normal_ranges_for_physiological_variables/
Sapra, A., Malik, A., & Bhandari, P. (2023). Vital sign assessment. StatPearls/NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK553213/
University of Iowa Health Care. (2017). Pediatric vital signs normal ranges. Iowa Head and Neck Protocols. https://iowaprotocols.medicine.uiowa.edu/protocols/pediatric-vital-signs-normal-ranges